ARTICLE
Gender, mental illness and the Hindu Marriage Act, 1955
Soumitra Pathare, Renuka Nardodkar, Laura Shields, Joske FG Bunders, Jaya Sagade
DOI: https://doi.org/10.20529/IJME.2015.003
Published online: December 10, 2014
ABSTRACT
Introduction: Section 5(ii) of The Hindu Marriage Act, 1955 (HMA) states that under certain circumstances, mental illness is accepted as a ground for the annulment of marriage, while Section 13(1) (iii) states that mental illness is a ground for divorce. There is little data on how this provision is used and applied in matrimonial petitions. This paper assesses judicial practices in divorce cases, exploring the extent to which gender and the diagnosis of mental illness affect the decision to grant annulment or divorce. Methods: The paper analyses judgments related to annulment and divorce at the Family Court in Pune and at the High Courts in India. Results: In the Family Court at Pune, 85% of the cases were filed by husbands, who alleged that their spouse was mentally ill. Medical evidence of mental illness was presented in only 36% of the cases and in many cases, divorce/nullity was granted even in the absence of medical evidence. In 14% of the cases, nullity/divorce was granted even when both spouses were not present. Of the Family Court cases reaching the High Court, 95% were filed by male petitioners. The High Courts reversed the lower courts’ judgments in 50% of the cases. Discussion: Our analysis highlights the need for standardised guidelines for lower courts on what constitutes adequate medical proof of mental illness when hearing a petition related to nullity or divorce under HMA. It also provides a critical review of Section 5(ii) of HMA.
INTRODUCTION
Marital disputes and family matters in India: the legal scenario
Family-related legal procedures in India are governed by personal laws, which are steeped in religious beliefs and cultural values. Across all religions, cases pertaining to matrimonial issues, maintenance, alimony and the custody of children, whether during marital disputes or after divorce, are tried by the Family Courts or by District Courts. Before Family Courts were introduced, the Code of Civil Procedure was amended with the aim of establishing a special procedure for proceedings related to matrimonial disputes. In 1974, the report of the Status of Women Committee (1), together with the report of the 59th Law Commission (2), recommended that the Central Government establish a separate judicial forum to settle family disputes.
Family courts were introduced in some parts of India through the Family Courts Act, 1984 (FCA), which was intended to be a part of the legal reforms related to the position of women in society. FCA enables the state government (in consultation with the High Court) to establish a Family Court in any area of the state which is a city, or in areas where the population exceeds one million. The idea behind the establishment of the Family Court and the separation of the functions of the Civil Courts was to expedite the settlement of family disputes (3). Although the central government issues the qualification criteria for the judges of Family Courts, the enforcement of FCA is governed largely by the High Courts, and thus, the Family courts are permitted to establish their own procedures.
A case filed at the Family Court goes up in appeal to the High Court and then to the Supreme Court. The High Court has jurisdiction over the entire state and has the legal power to transfer cases between Family Courts.
The role of Family Courts in Maharashtra
In Maharashtra, only 11 Family Courts (4, 5) have been established since 1987. It is important to note that Family Courts in the state have marriage counsellors, who are expected to counsel couples and preserve the institution of marriage. Social welfare employees may also be employed in specific cases. Although the original idea behind having a marriage counsellor was to protect women, counsellors have been criticised for working against the interests of women as they see their role as being that of preserving the institution of marriage at all costs. Interestingly, the reports prepared by marriage counsellors are not binding on the judiciary and are not cross-checked (3).
Nullity or divorce on the ground of mental illness
According to HMA, a marriage may be solemnised on the fulfilment of certain conditions, specified in Section 5 of the Act. When HMA was enacted in 1955, Section 5(ii) specified the condition that “neither party to the marriage should be an idiot or lunatic.” The Marriage Laws (Amendment) Act, 1976 amended HMA and substituted this clause with another one (in the current Section (ii) of the HMA), which states that a marriage may be solemnised if “at the time of marriage, neither party is (a) incapable of giving a valid consent to it in consequence of unsoundness of mind, or (b) though capable of giving a valid consent, has been suffering from mental disorder of such a kind or to such an extent as to be unfit for marriage and the procreation of children, or (c) has been subject to recurrent attacks of insanity or epilepsy”. The term “or epilepsy” was deleted from this sub-section in 1999. None of the terms used here, such as “unsoundness of mind”, “mental disorder” or “insanity”, are adequately defined.
Under sub-section 1(b) of Section 12 of HMA, a marriage is “voidable” and “may be annulled by a decree of nullity…if…the marriage is in contravention of the condition specified in clause (ii) of Section 5.” Thus, mental illness may form the ground for annulment of a marriage. Sub-section 1(c) of Section 12 allows for the annulment of a marriage if “the consent of the petitioner . . . was obtained by force, or by fraud as to the nature of the ceremony or as to any material fact or circumstance concerning the respondent.”Under this provision, petitioners may claim that the concealment of mental illness prior to marriage is a “material fact” and hence, seek annulment of the marriage on the ground of fraud.
Section 13 of HMA specifies grounds for divorce. In sub-section (1) (iii) of Section 13, mental illness is accepted as a ground for divorce under certain circumstances. The sub-section states that divorce is permissible if someone “has been incurably of unsound mind or has been suffering continuously or intermittently from mental disorder of such a kind and to such an extent that the petitioner cannot reasonably be expected to live with the respondent. “Section 13(1) has an “Explanation”, which states:”(a) the expression ‘mental disorder’ means mental illness, arrested or incomplete development of the mind, psychopathic disorder or any other disorder or disability of the mind and includes schizophrenia; (b) the expression ‘psychopathic disorder’ means a persistent disorder or disability of mind (whether or not including sub-normality of intelligence) which results in abnormally aggressive or seriously irresponsible conduct on the part of the other party, and whether or not it requires or is susceptible to medical treatment.”
These provisions of HMA are discriminatory against persons with mental illness as they make mental illness the only form of disability that can constitute a ground for the annulment of marriage or divorce. There is also a potential for the misuse of these provisions in a gender-biased manner. First, in a patriarchal society such as that of India, in which men are the sole decision-makers in the family, the equal enjoyment of rights and entitlements by women can be easily compromised. Second, the substantial stigma associated with mental illness reinforces the false notion that persons with mental illness are violent and dangerous to self or society and cannot be expected to continue in a marriage. Third, many people have the misconception that mental illness is associated with infertility and reduced childbearing capacity. This is reflected in Section 5(ii)(b) of HMA, cited earlier:”…though capable of giving a valid consent, has been suffering from mental disorder of such a kind or to such an extent as to be unfit for marriage and the procreation of children.“.Finally, the misconceptions regarding the genetic inheritance of mental illness may have a negative impact on the use of such provisions. Women with a mental illness may face double discrimination in cases related to marriage laws (6, 7)
The objective of this paper is to assess judicial practices to determine the role of gender and medical evidence in proceedings in matrimonial cases in at Family Court and High Courts.
To explore the issue, we conducted an analysis of judgments on annulment and divorce at the Family Court in Pune, focusing specifically on cases in which annulment or divorce was being sought on grounds related to unsound mind and/or mental illness (Section 12 (1)(b) and (c) and Section 13(1)(iii) of HMA). We also analysed cases related to annulment or divorce on the ground of mental illness that had been decided by various High Courts in India.
METHODS
We obtained permission from the Principal Judge at the Family Court in Pune to conduct this study. One faces major practical difficulties while searching for and retrieving cases in the Family Court. The data are not computerised, and all the physical data are stored in a record room and are not indexed. When a case is filed in the Family Court, the basic data (including the relevant Section of HMA under which annulment or divorce is being sought) are entered in writing in a register. These registers are maintained on a yearly basis. We first searched through the yearly registers and found details of cases in which the plaintiff had pleaded for annulment under Section 12(1)(b) or Section 12(1)(c) or divorce under Section 13(1)(iii). We then had to request the staff of the Family Court to dig out the relevant case papers. We were allowed to examine the case records and read through them. We were not permitted to take copies of the records or take them out of the records room. Although we had initially planned to search for cases spanning a 20-year period (1993–2012), it was logistically not possible for the staff to identify cases from earlier years. Therefore, this analysis covers only a 17-year period (1996–2012).
Further, it was only for 2011 and 2012 that we could collect the details of the total number of annulment or divorce cases filed. For all other years, it was possible to collect the details of annulment cases filed only under Section 12(1)(b) or Section 12(1)(c) or divorce cases under Section 13(1)(iii).
The data extracted from the case records were recorded manually and entered into an Excel spreadsheet. These data included information on: the date of marriage, date of separation, date of filing of the petition, date of the judgment, the person who had filed the petition (husband or wife), the type of relief sought, the type of medical evidence presented in the petition, and the final judgment of the court. No personal information that could be used for identification, such as the names, addresses (agree) and contact details, was recorded.
To look for cases at the High Court level, an electronic database search was conducted, using the Supreme Court Cases Database (SCC Online) and Indiankanoon.org and covering the period from 1976 (when HMA was amended) to 2013. The first relevant judgment yielded by the search was from the year 1981. Only those cases filed under the current HMA and those pleading for nullity or divorce on the ground of mental illness (Section 12 (1)(b) or 12(1)(c) or Section 13(1)(iii)) were included.
Descriptive statistics are presented as number and percentage. Where appropriate, statistical tests were performed using SPSS version 20 (IBM 2011). The chi-squared test of independence (X2) was used for categorical variables, and the significance level for all analyses was set at =0.05.
Results
Cases at the Family Court in Pune
Our search revealed that in all the annulment and divorce cases filed under HMA in 2011, 61% of the petitioners were husbands (n=753) and 39% wives (n=480). Similarly, in 2012, 60% of the petitioners were husbands (n=877) and 40% wives (n=575).
Our search specifically identified 78 petitions filed on the ground of mental illness under HMA from 1996 to 2012. Of these, 67 were filed by husbands and 11 by wives. Of the 78 petitions, 21 sought nullity (18 husbands and 3 wives), 50 sought divorce (43 husbands and 7 wives), and 5 sought nullity and/or divorce (4 husbands and 1 wife).In 2 cases (both husbands), the kind of relief (nullity/divorce) being soughtwas unclear. Surprisingly, husbands filed 85% of the petitions, whereas wives accounted for only 15% of the petitions filed on the ground of mental illness.
We looked for medical (psychiatric) evidence in the case papers or recorded in the judgment. Medical evidence is defined as any medical information, data, medical records or expert witness testimony which substantiates that the opposite party has a mental illness. We were able to find medical evidence in only 36% (28 out of 78) of the cases. In the case of male petitioners, medical evidence of the mental illness of the wife was present in 39% (26 out of 67) of cases, while in the case of female petitioners, it was present in only 18% (2 out of 11) of cases.
Table 1: Medical evidence presented at Family Court level
| Type of medical evidence | Witness-in-chief of psychiatrist | Certificate by psychiatrist | Prescript-ion | Invoices for purchase of medicines | Copies of medical reports | Multiple evidence* |
| Number of petitions filed by husbands | ||||||
| Annul-ment (n=6) | 1 (17%) | 1 (17%) | 4 (67%) | |||
| Divorce (n=19) | 4 (21%) | 1 (5%) | 3 (16%) | 1 (5%) | 10 (53%) | |
| Annul-ment and divorce (n=1) | 1 (100%) | |||||
In the 26 instances in which husbands provided medical evidence in the petition/court, prescription of psychotropic medicines was the only evidence in three cases, copies of medical notes were the only evidence in one case, and, invoices for the purchase of psychotropic medicines were the only evidence presented in one particular case. In the two instances in which wives provided medical evidence in the petition/court, multiple forms of evidence were presented (Table 1).
Nearly a fourth (22%) of the petitions filed by husbands without medical evidence of mental illness were successful and nullity or divorce was granted on the ground of mental illness. When husbands did present medical evidence of mental illness, a greater proportion of the petitions were successful (35%) and annulment or divorce was granted. Interestingly, a large proportion of the petitions which were not accompanied by medical evidence (43%) were converted into pleas for divorce by mutual consent (Table 2). Even when medical evidence was presented, a significant number of these petitions (31%) too were converted into divorce by mutual consent Table 2).
Table 2: Outcome of petitions filed by husbands, categorised by presence or absence of medical evidence
| Medical evidence provided | ||||
| Type of relief sought | Nullity(n=6) | Divorce (n=19) | Nullity and divorce (n=1) | Total (n=26) |
| Allowed (n, %) | 3 (50) | 6 (32) | 9 (35) | |
| Dismissed (n, %) | 1 (16) | 5 (26) | 6 (23) | |
| Converted to mutual consent (n, %) | 1 (17) | 6 (32) | 1 (100) | 8 (31) |
| Withdrawn (n, %) | 1 (17) | 1 (5) | 2 (8) | |
| Other (n, %) | 1 (5) | 1 (3) | ||
| Medical evidence not provided | ||||
| Type of relief sought | Nullity (n=12) | Divorce (n=24) | Nullity and divorce (n=3) | Total (n=41) |
| Allowed (n, %) | 4 (33) | 5 (21) | 9 (22) | |
| Dismissed (n, %) | 2 (17) | 3 (12) | 1 (33) | 6 (15) |
| Converted to mutual consent (n, %) | 3 (25) | 11 (46) | 2 (67) | 18 (43)* |
| Withdrawn (n, %) | 1 (8) | 5 (21) | 6 (15) | |
| Other (n, %) | 2 (17) | 2 (5) | ||
As for the nine petitions filed by wives who failed to provide medical evidence, divorce was granted on the ground of mental illness in two (22%) cases. A significant number of these petitions too (66%) were converted into divorce by mutual consent. Of the two cases in which the wives presented medical evidence of mental illness, one was successful and one was converted into divorce by mutual consent.
Of the six petitions filed by husbands for the annulment of marriage in which medical evidence was presented, three were allowed (Table 2).One of these was an ex parte decision. Of the 12 petitions filed for the annulment of marriage by husbands who had not presented medical evidence, the Family Court allowed annulment in four cases. One of these was granted exparte. Of the divorces granted to husbands who had presented medical evidence, two judgments were delivered exparte. Interestingly, in 80% (4 of 5) of the divorces granted to husbands who had not submitted medical evidence, the judgments were delivered exparte. In the case of both women petitioners granted divorce in the absence of medical evidence, the judgments were delivered exparte. One of the two women petitioners who did present medical evidence was granted divorce in her husband’s absence.
Cases in High Courts
Cases come up to the High Court when a party is not satisfied with the decision of the Family Court or the District Court (in areas where there are no Family Courts). We came across 97 High Court cases, starting from 1981 (the first relevant High Court case after the amendment of HMA was from 1981), in which nullity or divorce was sought on the ground of mental illness. The High Court judgments were first analysed according to whether or not the plaintiff had provided medical evidence. Medical evidence was taken to be present if it was mentioned in the High Court judgment and absent if not (Table 3).
Table 3: Outcome of petition by presence or absence of medical evidence
| Medical evidence provided | ||||
| Decision | Medical evidence presented (n=77) | No medical evidence presented (n=20) | ||
| Nullity or divorce granted by lower court, confirmed by High Court | 18 (23%) | 4 (20%) | ||
| Refusal of nullity or divorce by lower court, confirmed by High Court | 22 (29%) | 6 (30%) | ||
| Judgment of lower court overturned by High Court | 37 (48%) | 10 (50%) | ||
Surprisingly, there was no statistically significant difference in the judgments of the lower courts and the High Courts with respect to either the presence or absence of medical evidence, X2=0.10, p=0.95.
Table 4: Outcome of cases in High Courts
| Appellant at High Court | Appeal allowed or partly allowed | Appeal rejected |
| Husbands (n=46) | 16 (35%) | 30 (65%) |
| Wives (n=49) | 31 (63%) | 18 (37%) |
| Both spouses (n=2) | 2 (100%) | 0 |
A chi-square test for significance reveals that the rejection of appeals by the High Courts was significantly higher for husbands than for wives (X2=7.70, p=0.00), which perhaps indicates that women are more successful in having the family court’s judgment overturned (Table 4).
For all the High Court cases, we then explored who filed the original petitions at the Family Court/District Court and the outcome of the petitions at these courts. It is not practically possible to check the gender distribution of cases seeking nullity or divorce on the ground of mental illness in all Family Courts across the country, and we wanted to see whether the gender distribution of a sample of cases reaching the High Court from across the country would be similar to that found in the Family Court in Pune.
Table 5: Gender distribution and outcome of petition at lower court level
| Petitioner at Family Court/District Court (N=97) | Petition allowed | Petition rejected | Judicial separation |
| Husbands (n=92) | 46 (50%) | 43 (47%) | 3 (3%) |
| Wives (n=1) | 1 (100%) | 0 | 0 |
| Both (n=4) | 3 (75%) | 1 (25%) |
In 92 (95%) of the 97 cases, the husband filed the original petition. This is more than the 85% we found at the Pune Family Court, and shows that even in the case of petitions that had reached the High Court, it was the husbands who had filed most of them.
Table 6: Outcome at lower court of cases reaching High Court
| Decision | Medical evidence present (n=77) | Medical evidence absent (n=20) |
| Nullity or divorce granted | 42 (55%) | 8 (40%) |
| Nullity or divorce refused | 34 (44%) | 10 (50%) |
| Judicial separation | 1 (1%) | 2 (10%) |
Table 6 shows that 40% of the petitions were successful in the lower courts even in the absence of medical evidence; however, 50% of these judgments were subsequently overturned by the High Court (see Table 3).
Table 7: Reversal of lower courts’ judgments by the High Court
| Medical evidence present (n=77) | Petitioner | Success at Family Court/District Court | Appeal at High Court (HC) | Result | HC favoured |
| 18 petitions for nullity | 17 petitions filed by husbands | 13 petitions successful | 13 | 8 appeals allowed | Wives (n=7) and husband (n=1) |
| 5 appeals dismissed | Husbands (n=5) | ||||
| 4 petitions dismissed | 4 | 2 appeals dismissed | Wives(n=2) | ||
| 2 appeals allowed | Husbands (n= 2) | ||||
| 1 petition filed jointly by husband and wife | Petition allowed | 1 | Appeal allowed | Wife (n=1) |
Table 7 shows that while 13 of the 17 petitions filed by husbands were successful at the Family Court/District Court, the High Court reversed the lower courts’ decisions in more than 50% of cases.
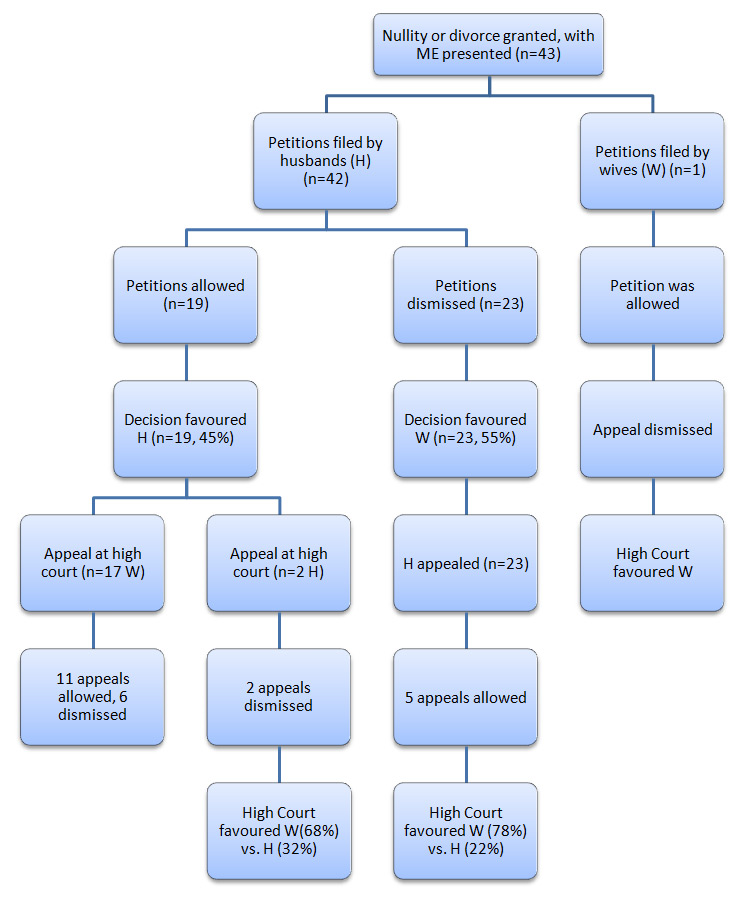
The High Court had overturned the lower courts’ judgment in the majority of cases in which medical evidence had been presented, in which the petitioner in the lower courtswas male, and in which the ruling was in favour of the husband and divorce had been granted (Figure 1). On the other hand, the High Court had upheld the lower courts’ judgment in a majority of the cases in which they had ruled against the husband and refused divorce (Figure 1). The High Courts had overturned the judgment of the lower courts when they had granted divorce in cases in which medical evidence was absent and the petitioner in the Family Court/District Court was the husband (e.g. 6 out of 7).
Table 8: Type of medical evidence (n=77)
| Nullity (n=18) | Divorce (n=43) | Both nullity and divorce (n=16) | Total (n=77) | |
| Witness-in-chief of psychiatrist(s) | 5 (28%) | 10 (23%) | 5 (31%) | 20 |
| Witness-in-chief of doctor(s) | 2 (11%) | 7 (16%) | 1 (6%) | 10 |
| Examination report | 2 (11%) | 2 (5%) | 3 (19%) | 7 |
| Examination report by medical board | 1 (2%) | 1 | ||
| Prescription | 1 (6%) | 1 | ||
| Referral letter/ admission/ discharge slip | 1 (2%) | 1 | ||
| Multiple evidence | 6 (33%) | 19 (44%) | 7 (44%) | 32 |
| Type of medical evidence not specified | 2 (11%) | 3 (7%) | 5 |
With regard to the type of medical evidence presented to substantiate the allegation of mental illness, it is interesting to note that the only evidence submitted in 10 of the 77 cases was a general doctor’s evidence. In one case, a prescription was the only evidence, and in another, a referral letter/discharge slip (Table 8).
DISCUSSION
This paper assessed the judicial proceedings and outcomes of divorce cases in Pune and explored the extent to which gender influences the decision to grant a divorce on the basis of mental illness. The analysis focused on annulment and divorce petitions and judgments at the Family Court in Pune and the High Courts nationwide.
We shall now discuss the three main findings of the analysis, as these merit further consideration. At the Family Court, 85% of the cases filed on the ground of mental illness were brought in by husbands. Further, of all petitioners who filed for divorce in general (ie not specifically on the ground of mental illness) in the Family Court, 61% were husbands. Similarly, of the cases that reached the High Court, 95% had originally been filed at the Family Court by male petitioners. If we take these findings in conjunction, it appears that more men than women file for divorce on the ground of mental illness, and perhaps use mental illness as a reason to seek divorce or nullity. This is possibly reflective of the difference in the standing of men and women with respect to marriage, and the intersection of disability with this factor. In this context, mention must be made of the socioeconomic anomalies between men and women, who, for example, are less likely than men to receive support for divorce from their natal families. In addition, they may not have the financial independence to feel confident enough to file for a divorce. Second, cultural expectations regarding a woman’s role in a marriage may influence the number of women who file for divorce. As Addlakha (8), Ghai (9) and others (10) state, a woman with a disability is considered incapable of fulfilling her duties as a wife, homemaker, mother, etc.
The second finding relates to whether or not medical evidence was presented in the petition or in court. Our analysis revealed that in the Family Court, medical evidence was presented in only a third of the cases, despite the fact that nullity or divorce can be granted only if the plaintiff can establish that his/her spouse has a mental illness. Divorce or nullity was granted in 22% of even those cases in which no medical evidence was presented. The corresponding percentage for cases in which medical evidence of mental illness was presented was only 35. Even when medical evidence was presented, it was often of poor quality and not fit to be considered as robust proof of mental illness. For example, in at least 20% of the 26 cases, simple prescriptions, copies of medical records, and invoices for the purchase of medicine constituted the sole piece of evidence and were accepted by the courts.
At the High Court level, too, no medical evidence was provided in nearly 20% of the cases. This finding is disconcerting as the High Courts reversed the judgment of the lower courts in only 50% of the cases in which no medical evidence was produced. It is inconceivable that the courts should make such decisions in the absence of substantial medical evidence. As in the case of the lower courts, the evidence presented before the High Courts was of poor quality. Unless clear guidelines are formulated on what is considered acceptable and sound medical evidence of mental illness, judicial practices are unlikely to change.
Our analysis also revealed that 11(14%) of the 78 judgments at the Pune Family Court were made under exparte conditions, despite the fact that the Madras High Court has explicitly stated that exparte judgments should not be delivered and proper representation is required (11)*.
An unexpected finding of our study was that a substantial number of the petitions for nullity or divorce on the ground of mental illness were converted into petitions for nullity or divorce by mutual consent. Though the underlying reasons for this are unclear and should be further explored, one could speculate that given the stigma associated with mental illness in the Indian context, the plaintiff may use the notion of “mutual consent” as a tool to pressurize his/her spouse into agreeing to a divorce. This would reduce the stigma, as mental illness is not documented in a judgment if the case involves mutual consent. This is not so if nullity or divorce is granted on the ground of mental illness. The documentation of the presence of mental illness in a judgment is problematic, since it could compromise any future chances of remarriage. This is because of the tendency to shun marital alliances with persons with disabilities (including mental illness), a tendency which is well documented both in the Indian context as well as other contexts (8, 10, 12, 13, 14).
Our analysis also found that the High Courts had overturned a large number of judgments of the lower courts, particularly in cases in which the petitioner was the husband and nullity or divorce had been granted. At the same time, the High Courts had confirmed the judgments of the lower courts in cases in which the latter had refused to grant divorce to a male petitioner. This means that the High Courts’ emphasis is on the preservation of marriage and/or supporting women, regardless of the presence or absence of a mental illness. This finding of our analysis has certain gender implications. Approximately 5%–6% of cases go up in appeal to the High Courts., Women, in particular, lack the resources to appeal to the High Court (15). The lack of financial resources is just one among many reasons that make women less likely to appeal to the higher courts. However, our data show that if women had the means to appeal, they would stand a good chance of having the judgment of the lower court reversed. High Courts appear to display greater gender sensitivity with respect to mental illness and marriage than do the Family and District Courts. Given that most cases do not go up to the High Courts, it is imperative to sensitise the lower courts to the social and gender aspects of the marriage laws with special reference to mental illness.
Broadly speaking, the language of HMA may also create conceptual confusion and be reflected in judgments. The phrase used in Section 13(1)(iii) is “incurably of unsound mind”. “Unsound mind” is a legal concept and does not have medical equivalence (16), while curability is a medical concept. It is difficult to understand what the drafters had in mind when referring to medical curability (or lack of it) with respect to a legal term (unsound mind). Further, the stigmatization of mental illness is likely to increase if the concept of unsoundness of mind can nullify or dissolve a marriage (15). The definitions of “mental illness” and “psychopathic disorder” used in HMA do not necessarily correspond with the medical definitions and understanding of these terms. In HMA, the term “psychopathic disorder” encompasses intellectual disability. This term is hardly found in modern medical literature, which tends to use the term “personality disorder”. Besides, many concerns have been articulated in medical literature regarding the diagnosis of personality disorder, particularly the validity and reliability of the diagnosis (17, 18, 19, 20). Personality disorders have long been described as deviance from social norms and values. In the context of India, where patriarchal norms prevail, any challenge to male authority can potentially be labelled as a personality disorder. This may partly explain why a disproportionate number of female spouses are labelled as having a mental illness in divorce cases.
Taken together, the findings presented in this paper have a number of implications for policy, practice and future research. First, there is a need for uniform guidelines for lower courts on what can be accepted as adequate medical proof of mental illness. Also, proof of mental illness must be required when a petition seeks nullity or divorce on this ground under HMA. Second, there is a need for greater awareness and more research on this topic so that a sizeable evidence base may be gathered to push for the amendment of HMA. Such evidence could be used to consider the deletion of Section 5(ii) and Section 13, as these appear to be used in a gender-discriminatory manner. Their application is detrimental to the interest of women, and also does not fit with the modern understanding of mental illness and its curability or otherwise, taking into account the recent Supreme Court judgment (21). Further, it clearly violates the UN Convention on Rights of Persons with Disabilities, to which India is a signatory and is thus bound to implement the Convention in its domestic legislation. Third, the judiciary must be made aware of the need to adopt a more gender-sensitive approach to mental illness and divorce. Sensitisation activities should focus on the complex social, legal, cultural and medical factors that play a role in the use of mental illness as a ground for divorce in the Indian context. Finally, it would be interesting if future research could determine whether such patterns of the use of mental illness as a ground for divorce exist in other Family Courts in India, and even in South Asia. Data could be accumulated and fed into potential theoretical frameworks on mental illness and marriage (and divorce), thus strengthening the evidence that could then be used to facilitate advocacy and prompt an amendment to HMA.
Competing interests and funding support: The authors declare that they have no competing interests and have not received any funding to conduct this study. The authors are grateful to the Pune Family Court for granting them access to the petitions for the purposes of this study.
This article was published online on December 10, 2014, at ijme.in.
* Corrections have been made in the placing of references, with the previously numbered Reference no. 21 now no.11, and all subsequent references re-numbered accordingly.
References
- Committee on the Status of Women in India. Towards Equality: Report of the Committee on the Status of Women in India [Internet]. New Delhi: Government of India, Ministry of Education & Social Welfare; 1974 [cited 2014 Dec 7], 199 p. Available from: http://pldindia.org/wp-content/uploads/2013/04/Towards-Equality-1974-Part-1.pdf
- Law Commission of India. 59th Report on Hindu Marriage Act, 1955 and Special Marriage Act, 1954 [Internet]. New Delhi: Law Commission of India; Mar 1974 [cited 2014 Dec 7], 131 p. Available from: http://lawcommissionofindia.nic.in/51-100/Report59.pdf
- National Commission for India. Family Courts- Report on Working of Family Courts and Model Family Courts [Internet]. 20 Mar 2002 [cited 2014 Dec 7], p. 61. Available from: http://ncw.nic.in/pdfReports/Working%20of%20Family%20courts%20in%20India.pdf
- Law and Judiciary Department (including all offices) State Government of Maharashtra. Performance Budget (2013-2014) [Internet] [cited 2014 Dec 7]. 66-B p. Available from: https://www.maharashtra.gov.in/pdf/Budget/Law%20and%20Judiciary%20Department.pdf
- Times of India. Nanded city gets its first family court. The Times of India, Aurangabad [Internet]; 2014 Mar 31 [cited 2014 Dec 7]; Available from: http://timesofindia.indiatimes.com/city/aurangabad/Nanded-city-gets-its-first-family-court/articleshow/32988183.cms
- Sharma I, Pandit B, Pathak A, Sharma R. Hinduism, marriage and mental illness. Indian J Psychiatry. 2013 Jan [cited 2014 Aug 12];55(Suppl 2):S243-S249. doi:10.4103/0019-5545.105544
- Nambi S. Marriage, mental health and the Indian legislation. Indian J Psychiatry. 2005 Jan-Mar; [cited 2014 Dec 7]; 47(1): 3-14. doi:10.4103/0019-5545.46067.
- Addlakha R. Gender, subjectivity, and sexual identity: how young people with disabilities conceptualise the body, sex, and marriage in urban India. New Delhi:Centre for Women’s Development Studies; 2007, 46 p.
- Ghai A. Towards understanding disability. Psychol Stud. 2000 Nov;45(3):145-9.
- Talking About Reproductive and Sexual Health Issues (TARSHI). Sexuality and disability in the Indian context [Working paper]. 2000.
- A. Abitha v.Eben Jayanth C.R.P. (NPD) MD No. 1551 of 2011.
- Hinshaw SP. The mark of shame : stigma of mental illness and an agenda for change. Oxford University Press; 2006. 352 p.
- Thara R, Srinivasan TN. How stigmatising is schizophrenia in India? Int J Soc Psychiatry. 2000 Summer;46(2):135-41.
- Lauber C, Rössler W. Stigma towards people with mental illness in developing countries in Asia. Int Rev Psychiatry. 2007 Apr;19(2):157-78. doi: 10.1080/09540260701278903
- Sagade J. Law of maintenance: an empirical study. Pune: Indian Law Society; 1996: 224 p.
- Dhanda A. Legal order and mental disorder. New Delhi: Sage Publications; 2000: 356 p.
- Clark LA, Livesley WJ, Morey L. Special Feature:Personality disorder assessment: the challenge of construct validity. J Persl Disord. 1997 Fall;11(3):205-31.
- Clark LA. Assessment and diagnosis of personality disorder: perennial issues and an emerging reconceptualization. Annu Rev Psychol. 2007;58:227-57.
- Moran P. Should psychiatrists treat personality disorders? Maudsley Discussion Paper No 7. Institute of Psychiatry, King’s College, London.1999.
- Scott S. The medicalisation of shyness: from social misfits to social fitness. Sociol Health Illn. 2006 Mar;28(2):133-53.
- Kollam Chandra Sekhar v. Kollam Padma Latha. 2008 1 SCC 225.