ARTICLE
Nursing error: an integrated review of the literature
Mohaddeseh Mohsenpour, Mohammadali Hosseini, Abbas Abbaszadeh, Farahnaz Mohammadi Shahboulaghi, Hamidreza Khankeh
Published online: December 5, 2016
DOI: https://doi.org/10.20529/IJME.2017.020
Abstract
Nursing errors are complex and take place frequently in the care of patients. However, despite their significance, they have not been properly defined or addressed in the literature. This integrative review of the literature explored the concept of nursing error, explained its definitions and described its attributes and measurements. The databases of Medline, CINAHL, Google Scholar and SID were searched using a number of keywords, including malpractice, adverse events and mistake, with and without the word nurse. The aim was to determine the definition of nursing error, regardless of the contextual aspects, in various scientific systems. After reviewing the relevant literature, content analysis (in MAXQDA) was applied to classify the definitions, attributes and measurements obtained on the basis of their similarities and differences. Ultimately, a definition was established for the concept of nursing error.Introduction
The safety of the patient is a key component of the quality of care (1, 2, 3) and a critical concern in any healthcare system (4, 5, 6). Errors, on the other hand, are an integral part of human and professional life (6, 7).Though medical and nursing errors are inevitable and common, they are serious and a major threat to the patient’s safety (8, 9). The incidence of errors is high in health systems worldwide (3, 10, 11) and they affect about one out of every 10 hospitalised patients (6, 12, 13). Moreover, nearly 7% of these errors are fatal (12). While there are no official statistics on the incidence of medical errors in Iran (9), descriptive studies have suggested similar rates in this country (14, 15). Meanwhile, the increasing number of complaints filed about medical errors indicates the growing public awareness of the issue (9). The term “error” entails “deviation from correctness” and “taking the wrong path” (10). Lewis et al (2013) described nurses’ involvement in errors as an ambiguous problem requiring explanation (16). Medical errors occur when care providers make the wrong decision or use the wrong procedure (8). Criminal law defines medical errors as the failure to meet diagnostic, therapeutic and care standards. In legal literature, failure is categorised as either negligence or violation of the rules (10). However, individuals studied by Sanagoo et al (2012) defined medical error as an act endangering the patient’s life or causing any kind of harm to the patient (17). This is drastically different from the legal definition. Nursing aims to help vulnerable people. Caring is thus an entirely moral action (18). An incorrect act will cause additional harm to a vulnerable person. Since detrimental actions create turmoil in the minds of nurses, they try to avoid such actions (18, 19). While various scientific, ethical and legal references have described error (sometimes using complex and vague definitions), nursing error, in its professional sense, has not been well defined. Therefore, our study aimed to shed light on this concept. Since we aimed to focus on various definitions, attributes and consequences of nursing errors rather than the effects of an intervention or the frequency and incidence of a particular concept, we conducted an integrative review as a concept analysis method (20), which is a specific method for summarising the evidence available and clarifying a health issue or phenomenon (20, 21).Objective:
Concept analysis of nursing error by integrative reviewMethods:
Our study adopted the integrative review method: a systematic rigorous method of concept analysis to review scientific literature using diverse methodologies with specific aims. The integrative review process generally involves concept identification and a research question, a search of the literature, evaluation of data, data analysis, and the presentation of results (20, 21).Concept identification and research question
This stage consists mainly of the identification and formulation of the problem and the objective of the review (21). As we sought to develop a clear and scientific definition of the concept of nursing error, we stated the research question as: “how nursing errors can be defined, irrespective of the contextual aspects of various scientific systems”.Search of the literature
During the second stage of an integrative review, a well-defined method is used to make a broad systematic interdisciplinary search of the literature available on the basis of the research question (21). In our study, the Google search engine was used to search Persian websites. For references on topics related to medical ethics, law and jurisprudence, we manually searched the whole series of the Iranian Journal of Medical Law and the Quarterly Journal of Medical Figh, available at the Medical Ethics and Law Research Centre of Shahid Beheshti University of Medical Sciences, Tehran, Iran. Several databases, including Medline, CINAHL (PubMed) and Google Scholar, were searched, using the keywords “errors”, “malpractice”, “adverse events” and “mistakes”, with and without the word “nurse”. We also searched the Scientific Information Database (a comprehensive data bank in Iran), using the keywords “error”, “mistake” and “negligence”, with and without the word “nurse”, between 1990 till 2015.In addition, the titles, abstracts and keywords of articles were searched for the keywords. The same procedure was followed when the researchers came across a new synonym for “error” in the literature. The search procedure finally yielded 1924 articles (Fig. 1).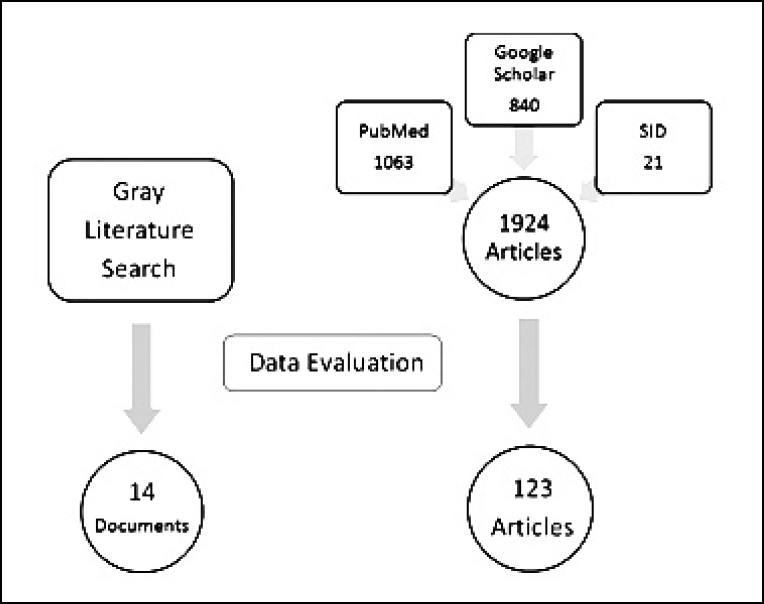
Figure 1: Literature search process
Evaluation of data
The relevance of the extracted articles to the study question was evaluated by the assessment of their abstracts. In case of any ambiguity, however, the full text of the article concerned was reviewed. Articles containing appropriate answers to the research question (eg implicit or explicit definitions, antecedents, consequences, attributes, or measurements of nursing or other healthcare team errors) were identified and entered in MAXQDA (VERBI, Berlin, Germany) as the unit of analysis. Books and articles without an existing computer file were analysed manually. In total, 137 documents, including 123 full text articles, 2 theses, 3 reports, 7 books, one Internet page (MeSH term), and the Islamic Penal Code (notified in April 2013), were analysed.Data analysis
Content analysis was used to analyse the literature. A number of meaning units, including the implicit and explicit definitions of nursing error, and the attributes, antecedents, consequences and measurement of the concept, were identified as codes in the article texts. These codes were then categorised on the basis of similarities and contrasts. Accordingly, the categories were grouped into themes. The attributes, antecedents and consequences of nursing error were presented as follows.Results
The results were comprehensively expressed and appropriate explanations were provided to facilitate a general understanding of them (21). To clarify the concept of nursing error, the data were reduced to seven themes, including nursing error as a concept based on outcome (with three sub-themes, namely definitions based on adverse events, legal definitions and goal-based definitions), on process, on cognitive reasoning, and on ethics, and nursing error characteristics, antecedents, and consequences.Attributes of nursing errors
Several important attributes of nursing errors are mentioned in the literature. In brief, nursing errors are a “preventable” yet “unavoidable” challenge (13, 22, 23). They are preventable since their incidence should not be attributed to chance. On the other hand, nursing errors are unavoidable because appropriate and targeted measures can merely reduce their incidence, and not negate the probability of their occurrence (24). In fact, the only way to avert nursing errors is to avoid tasks, which is not possible in nursing. The inadvertent nature of nursing errors was also emphasised in all definitions (22, 25). More precisely speaking, an error occurs when a nurse aims to benefit the patient, ie acts of malice, malevolence and profiteering are not considered nursing errors (22, 26). It is, however, important to mention that errors may occur either consciously or unconsciously, and deliberate errors are not categorised as nursing errors. For instance, while a nurse may know that inserting an intravenous line for a patient with dementia requires the informed consent of the latter’s guardian, she/he may perform the task with the patient’s consent considering the significance of drug timing. In this case, a conscious, benevolent error is committed without the intention to harm the patient. Nursing error has negative connotations (16, 24, 25). In other words, a degree of deviation is involved in all nursing errors, no one benefits from or seeks errors, and errors have no direct favourable consequences. The multiplicity of the terminologies related to nursing error and the several definitions of the term reflects the complexity of the concept (10, 24). The situations in which nursing errors occur are very complicated and to analyse them, one must consider the cause of the error, environmental factors, theories of behaviour, the prevailing perceptions, anticipation of human error, and ethical theories. The best fitting definition of nursing error is clear in some situations, but this definition need not be as valid in other circumstances. Nursing errors are human operations (24), iea human being, in this case a nurse, must be involved in their occurrence (16). Further, they have to be caused during the process of the provision of care and when the wrongdoer is in charge of such care. Finally, several (at least two) options must be available for a nursing error to take place, ie such errors are meaningless if a choice is not made.Nursing error as an outcome-based concept
This theme emphasises unachieved outcomes of care or unintended outcomes caused by the omission or commission of acts of care (3, 13, 22, 24, 25, 27). According to such definitions, nursing error can be defined as the commission of wrong care or the omission of care, both of which lead to unintended outcomes or are likely to lead to an unfavourable outcome(28, 29, 30). This category comprises two main subcategories, as follows.- Definitions based on adverse events: According to these definitions, an error occurs when the medical management of a patient results in adverse consequences (3, 22, 24, 25, 27, 31), eg harm, prolonged hospitalisation, measurable disability and death, or certain other conditions that can lead to such consequences. Outcome-based definitions, the first published definitions of medical errors, were put forward in a study of the side-effects of treatment by Moser in 1956 (24) and a statement by the US Institute of Medicine, “To Err Is Human”, issued in 1999 (32). The definition by Medical Subject Headings was also one of the early definitions of medical error in this group.
- Goal-based definitions: In this group of definitions, the goal of care is seen as the only yardstick of the consequences of care and hence, error. Any deviation from achieving the intended goal is thus considered a nursing error (23, 26). More precisely, this group of definitions assumes the goal of care to be authentic within a predetermined framework. Therefore, any deviation from this framework is regarded as a nursing error if it prevents the complete achievement of the goal (23). Unlike the definitions based on adverse effects, an action which leads to an outcome (even if not adverse) that is different from the intended goal is considered an error here.
Nursing error as a process-based concept
According to this group of definitions, errors are caused by faulty planning for the achievement of a goal or the misconduct of a well-designed plan (3, 10, 13, 22, 25, 34, 35). The definitions based on the action theory of Volpert (1992) and Hacker (1998) can be placed in this category (23). According to these definitions, any action comprises hierarchical and sequential components and can thus be expressed as a hierarchy of operations (23). Since any operation is considered to consist of several sub-goals, the failure to achieve one of these sub-goals or a disturbance in the hierarchy or sequence of operations and their sub-goals would lead to an error. This group of definitions emphasises standards as the indicators of performance. Therefore, actions that do not conform with the standards are identified as nursing errors (10, 13, 23). In other words, since what has been done is compared with what should have been done, a nursing error occurs when a nurse chooses the wrong procedure of care or performs the right procedure incorrectly (3). In contrast to outcome-based definitions, process-based definitions see such deviations as errors, regardless of the presence/absence of harm to the patient. Not only human factors, but also environmental and organisational factors are involved in nursing errors. Since definitions based on these factors focus on the standards and quality of care, they are not comprehensive and exclusive, and intersect with context-based definitions. As a result, the definition of nursing errors will depend on that of standards and the failure to follow them. Some of these definitions describe the standard as the average actions that a normal nurse is assigned. Hence, actions that are below average or are irrelevant to the duties assigned are considered nursing errors. Some other definitions in this group mention the judgment of expert colleagues as a criterion for the standard. It is also essential to incorporate the factor of time into the definitions. In other words, due to the technological and scientific advances and theclinical facilities available, an action which may not be regarded as a nursing error at a particular time can be seen as one at another time.Nursing error as a concept based on cognitive reasoning
In these definitions, nursing error is described in terms of an incorrect cognitive process of assessing a situation when achieving a goal (10, 23, 36, 37). Since an error is considered the result of a disruption in cognitive reasoning, these definitions focus on “accuracy” and can thus link goal-based and process-based definitions (24, 38, 39, 40). The proponents of this view believe that a behaviour takes place in a state of functioning that can be described as either the attentional mode or the automode. Since tasks are performed cautiously in the attentional mode, this state is slow and mental effort is required to use newly learnt skills. When the same task has been repeated often, the brain gradually switches to automode to prevent exhaustion. There is a chance of the occurrence of various errors during both states. Apparently, these definitions consider not only goals, but also plans to achieve these goals. However, they concentrate only on human causes and ignore other possible causes.Nursing error as an ethical concept
From the ethical standpoint, nursing error is a broad phenomenon which does not necessarily concern harm to the patient. Instead of defining an error as a deviation from the only existing correct way, ethics generally focuses on better or more fitting choices (10, 26). In other words, when ethics is involved, there are no guidelines to violate. Since quality is an indefinite range, there is a better option for any particular choice. Hence, it is critical to know how fitting a specific choice has been under the circumstances in which it was made. Obviously, in contrast to the legal definition of nursing error, ethics judges an error on the basis of the individual’s conscience rather than the extent of harm caused.Nursing error as a contextual concept
As an abnormal behaviour, nursing error depends profoundly on how norm is defined. The definition of norm, however, varies in different contexts (3, 13, 24, 25). Norm can be defined on the basis of religion, culture, beliefs and lifestyle. For example, due to differences in religious beliefs or world views, euthanasia is a norm in some countries and is objectionable in others. Most studies on medical errors in developing countries concentrated on adverse events (28, 29, 30, 31, 37, 41). There is a lack of clarity regarding the concept of nursing error, which is not understood by healthcare systems in the developing countries in all its aspects. Various studies have tried to incorporate the effects of context into the definition of error. Some researchers have defined nursing error on the basis of the judgement of expert peers (26, 42). They argue that when there is an absolute consensus on the occurrence of an error (eg if 20 out of 20 nurses agree that it is nursing error), an error has definitely occurred. Several other studies have established a link between contextual effects, perspectives on care, philosophy and theories (10, 13). They claim that one’s view of the world affects one’s understanding of right and wrong. Determinists contend that all events are caused by nature, chance or destiny, rather than human action. They thus render the issue of nursing error meaningless. On the other hand, according to the post-modern view, events are definitely the result of human decisions and behaviours. Therefore, instead of chance or bad luck, care providers are to be blamed for unintended events in healthcare. According to Dekker, healthcare has both social and technical contexts (24). The context may be affected by differences in the characteristics of the professionals and nurses concerned. Nurses who have committed an error may have a different understanding of nursing error not only because of cultural differences, but also because of their training regarding error, workplace conditions and the amount of attention paid to errors in their organisation. Some context-based definitions of nursing error also consider the effects of time. Thus, with changes in the accepted theories of care and the facilities available, something which may not be considered a nursing error at one time may come to be regarded as one at another time. For example, the guidelines for dressing methods are revised every year in a hospital. If a nurse follows the previous year’s guidelines, he/she is committing a nursing error even though it was not an error a few days ago. The same goes for the replacement of instruments by the latest or best ones, or changes in theories or philosophies of care. According to the philosophy of the healthcare system, euthanasia may constitute an error but if this philosophy changes over time, it may become the norm. The fact that the definition of nursing error depends on rules and standards of care emphasises its context-based nature (10, 13, 23, 33). Since various organisations and countries formulate their own sets of rules and standards, it is apparently not feasible to develop a unique definition. The diversity of definitions makes the evaluation of the concept of nursing error a challenging task. Finally, patients’ understanding of nursing error, which too is completely culture-dependent, can affect not only the nurses’ perception, but also the general definition.- Legal definition of nursing error in Iran: In legal terms (Islamic Panel Code of Iran), negligence in the provision of nursing care is categorised as irresponsibility and inattentiveness (43, 44, 45). Two components of these are incompetence and non-compliance with governmental provisions. Irresponsibility involves the omission of a technically and scientifically expected act (eg injection with a non-standard needle, leading to drug leakage and the need for surgery). Inattentiveness refers to actions which are not scientifically expected (eg intravenous injection of a drug that is not to be administered through the intravenous route and causes seizure or death). Incompetence refers to actions performed by inadequately experienced or skilled individuals (eg subcutaneous injection of fluids, resulting in necrosis or skin graft). Noncompliance with governmental provisions is described as the violation of nursing duties as declared by the Ministry of Health (eg failure to protect the patient’s privacy, failure to take a decision under emergency conditions, and refusal to provide high-risk patients with the required care). Such violations are evaluated by the board of magistrates and the Provincial Appeal Board, which then impose disciplinary measures, including a verbal/written reprimand and short- or long-term suspension, on the wrongdoer.
Antecedents of nursing errors
Previous studies have adopted two main approaches to the identification of the causes of nursing errors (36, 46, 47). These approaches were presented by Reason (1990) who made a comprehensive classification of the antecedents of medical errors (48). The personal approach highlighted the personal factors (associated with the healthcare team and patients) related to nursing errors. The factors associated with the healthcare team included inexperience and young/old age of the nurse or doctor, the inability to give complicated or urgent care, poor communication (differences in language and medical terminology, lack of knowledge of the local language, incorrect reports and illegible handwriting. The factors related to patients that were viewed as nursing errors included the limitations faced by them and the presence of a relative to perform some of the tasks of care giving. In some cases, patient behaviours, eg patient falls, were also considered nursing errors. The organisational approach, described by numerous studies (22, 46), underscored the organisational (managerial) causes of nursing errors. This approach emphasised lack of coordination between teams, a crowded workplace, similarities in the names or appearance of medicines and poor equipment. There is greater interest in the organisational factors than the personal ones since they can be modified more easily and it is more practical to identify them. In addition, due to the negative connotation of nursing errors, the organisational factors are used to direct the blame from the wrongdoer towards the organisation.Consequences of nursing errors
According to the review of the literature, the consequences of nursing care could be categorised as human, financial, organisational and professional (16, 32, 46). The human consequences have an impact not only on the patients and their families, but also on the nurses and other professionals involved in the error. As a result of nursing errors, patients may suffer from death or disability, or may have to prolong their stay in hospital. Further, nurses and other professionals may experience distress, feelings of guilt, anger, shame or inadequacy, depression, and a loss of self-esteem. In addition, they may develop personality defects, face stigma, or change their job or field of study (16, 33, 49, 50). Research carried out earlier has indicated that patients and the medical team are the first and second victims, respectively, of nursing errors (49, 51, 52). The human consequences of nursing errors are generally irreversible. The financial fallouts of nursing errors affect patients and their family, responsible nurses and health organisations (25, 47, 53). Because of the need to prolong the hospital stay and changethe treatment plan, patients and their family have to pay additional costs (47, 53). Responsible nurses also have to bear a financial burden because they have to take leave from work (due to the legal and emotional complications following the error) and the costs incurred (eg compensation for the cost of treatment). Finally, health and insurance organisations will be required to cover some of the costs arising from the nursing error. Among the organisational consequences of nursing errors reported in the literature were damage to the system, loss of the hospital’s reputation, legal disputes and an increase in costs. The professional consequences included temporary or permanent loss of professionals after the occurrence of the error and damage to the professional image. Though researchers deem errors necessary (although very costly) for the dynamics of a system (24), it is to be noted that all the consequences of nursing errors are unpleasant. However, an appropriate defence mechanism against such unpleasant occurrences can produce positive effects. For example, learning from mistakes and reducing the frequency of nursing errors would be of some help. The unpleasant nature of nursing errors cannot prevent their recurrence, that is, in the absence of effective strategies, such errors would remain unreported and no lesson would have been learnt from them. According to previous studies, slight errors are unavoidable; but belief in the reversibility of errors and the relation between the level of shame and the degree of harm caused can contribute to reduction of the mentioned unpleasantness in preventing nursing errors. Finally, according to all the aspects of the concept of nursing error mentioned above, nursing error may be defined as follows.Nursing errors arecomplex, unintentional, preventable, yet unavoidable occurrences in which a nurse’s choice regarding whether or not to take a particular action for the patient’s care has adverse human, financial, organisational and/or professional consequences. An inappropriate choice may be the result of personal or organisational factors and can be interpreted differently on the basis of time and context.We have attempted to arrive at this definition on the basis of all the aspects of nursing errors described in the literature but, as we mentioned, the concept of nursing error is also viewed in the context of time and culture. Any definition of this concept, however comprehensive, has its limitations. It would be useful to carry out other studies focusing on the contextual aspects of nursing error to better understand this important clinical concept.
Conclusion
We have attempted to develop a comprehensive definition of nursing error by classifying and discussing the definitions available in the literature. The definitions of nursing error in the literature were classified into five main themes. Nursing errors were categorised on the basis of their outcomes, the care-providing process, the cognitive reasoning of nurses, and ethical and contextual aspects. The definition that we finally arrived at has its implications and limitations. The fact that “nursing errors” has been considered as an independent concept in this study is valuable. Competing interests and funding support This paper is the result of M Mohsenpour’s doctoral dissertation, which was supported and copyrighted by the University of Social Welfare and Rehabilitation Sciences. The authors have no conflicts of interest to declare.Acknowledgement
We appreciate the support of the Medical Ethics and Law Research Center of Shahid Beheshti University of Medical Sciences and of all those who helped us with this study.References
- de Neef M, Bos AP, Tol D. Safety as a criterion for quality: the critical nursing situation index in paediatric critical care, an observational study. Intensive Crit Care Nurs. 2009;25(6):341-7. doi: 10.1016/j.iccn.2009.08.002.
- Durmus SÇ, Keçeci A, Akkas Ö, Keskin S, Demiral N, Saygan S. Medical errors: an important indicator of quality of care and patient safety. Holist Nurs Pract. 2013;27(4):225-32. doi: 10.1097/HNP.0b013e318294e6d3.
- Garrouste-Orgeas M, Philippart F, Bruel C, Max A, Lau N, Misset B. Overview of medical errors and adverse events. Ann Intensive Care. 2012;2(1):2. doi:10.1186/2110-5820-2-2.
- Teng CI, Chang SS, Hsu KH. Emotional stability of nurses: impact on patient safety. J Adv Nurs. 2009;65(10):2088–96. doi: 10.1111/j.1365-2648.2009.05072.x.
- Tanaka K, Takahashi M, Hiro H, Kakinuma M, Tanaka M, Kamata N, Miyaoka H. Differences in medical error risk among nurses working two-and three-shift systems at teaching hospitals: a six-month prospective study. Ind health. 2010;48(3):357-64.
- Schwappach DL, Boluarte TA. The emotional impact of medical error involvement on physicians: a call for leadership and organisational accountability. Swiss Med Wkly. 2009;139(1-2):9-15. doi: /aop/smwaop12417.
- Martinez W, Lo B. Medical students’ experiences with medical errors: an analysis of medical student essays. Med Educ. 2008;42(7):733-41. doi:10.1111/j.1365-2923.2008.03109.x.
- Grober ED, Bohnen JM. Defining medical error. Can J Surg. 2005;48(1):39-44.
- Hashemi F, Nikbakht Nasrabadi A, Asghari F. Factors associated with reporting nursing errors in Iran: A qualitative study. BMC Nurs. 2012;11:20. doi: 10.1186/1472-6955-11-20.
- Crigger NJ. Always having to say your’s story: an ethical respose to making mistakes in professional practice. Nurs Ethics. 2004;11(6):568-76.
- Hashemi F, Nikbakht Nasrabadi A, Asghari F. Nurses perceived worries from error disclosure: a qualitative study. Iranian Journal of Nursing Research. 2011;20(6):30-43.
- de Vries EN, Ramrattan MA, Smorenburg SM, Gouma DJ, Boermeester MA. The incidence and nature of in-hospital adverse events: a systematic review. QualSaf Health Care. 2008;17(3):216-23. doi: 10.1136/qshc.2007.023622.
- Valiee S, Peyrovi H, Nasrabadi AN. Critical care nurses’ perception of nursing error and its causes: a qualitative study. Contemp Nurse. 2014;46(2):206-13. doi: 10.5172/conu.2014.46.2.206.
- Cheraghi M, Nikbakht Nasrabadi A, Mohammadnejad E, Salari A, Ehsani R. Medication errors among nurses in intensive care units (ICU). J Mazandaran Univ Med Sci. 2012 (1390);21(1):115-9.
- Hajibabaee F, Joolaee S, Peyravi H, Haghani H. The relationship of medication errors among nurses with some organizational and demographic characteristics. Nursing Research. 1390 (2011);20(6):83-92.
- Lewis EJ, Baernholdt M, Hamric AB. Nurses’ experience of medical errors an integrative literature review. J Nurs Care Qual. 2013;28(2):153-61. doi:10.1097/NCQ.0b013e31827e05d1.
- Sanagoo A, Majnoni M, Jouybari L, Ghana S, Kalantari S. Studying the nursing students experiences of clinical errors and dealing with them. Iranian Journal of Nursing Research. 1391 (2012);25(7):45-53.
- Borhani F, Abbaszadeh A, Mohsenpour M. Nursing students’ understanding of factors influencing ethical sensitivity: a qualitative study. Iran J Nurs Midwifery Res. 2013;18(4):310-5.
- Borhani F, Abbaszadeh A, Mohsenpour M, Asadi N. Lived experiences of pediatric oncology nurses in Iran. Iran J Nurs Midwifery Res. 2013;18(5):349-54.
- Rodgers BL, Knafle KA. In: Concept development in nursing fundations, techniques, and applications. 2nd ed. philadelphia: WB Saunders company; 2000.
- Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs. 2005;52(5):546-53.
- Eslamian J, Taheri F, Bahrami M, Mojdeh S. Assessing the nursing error rate and related factors from the view of nursing staff. Iran J Nurs Midwifery Res. 2010;15(Suppl 1):272-7.
- Bauer J. Learning from errors atwork. Studies on nurses’ engagement in error-related learning activities. Regensburg: University at Regensburg;2008.
- Armitage G. Human error theory: relevance to nurse management. J NursManag. 2009;17(2):193-202. doi: 10.1111/j.1365-2834.2009.00970.x.
- Grober ED, Bohnen JM. Defining medical error. Can J Surg. 2005;48(1):39-44.
- Hashemi F. Ethical response to nursing errors. Iranian Journal of Medical Ethics and History of medicine. 2007;4(1):31-46.
- Anderson O, Davis R, Hanna GB, Vincent CA. Surgical adverse events: a systematic review. Am J Surg. 2013;206(2):253-62. doi: 10.1016/ j. Am j surg. 2012.11.009.
- Kim CH, Kim M. Defining reported errors on web-based reporting system using ICPS from nine units in a Korean university hospital. Asian Nurs Res (Korean Soc Nurs Sci). 2009;3(4):167-76. doi: 10.1016/S1976-1317(09)60028-1.
- Kim J, An K, Kim MK, Yoon SH. Nurses’ perception of error reporting and patient safety culture in Korea. West J Nurs Res. 2007;29(7):827-44.
- Kim M. The effectiveness of error reporting promoting strategy on nurse’s attitude, patient safety culture, intention to report and reporting rate. J Korean AcadNurs. 2010;40(2):172-81. doi: 10.4040/jkan.2010.40.2.172.
- Kim J, Bates DW. Results of a survey on medical error reporting systems in Korean hospitals. Int J Med Inform. 2006;75(2):148-55.
- Benner P, Malloch K, Sheets V, Bitz K, Emrich L, Thomas MB, Bomen K, Scott K, Patterson L, Schwed K, Farrell M. TERCAP: creating a national database on nursing errors. Harvard Health Policy Review. 2006;7(1):48-63.
- Crigger NJ, Meek VL. Toward a Theory of Self-Reconciliation Following Mistakes in Nursing Practic. J Nurs Scholarsh. 2007;39(2):177-83.
- Bauer J, Mulder RH. Conceptualisation of learning through errors at work: a literature review. Emerging perspectives of workplace learning / edited by Stephen Billett, Christian Harteis and Anneli Etelapelto. Rotterdam, Netherlands: Sense Publishers; 2008.
- Borhani F, Hosseini S, Abbaszadeh A. Commitment to care: a qualitative study of intensive care nurses’ perspectives of end of life care in an Islamic context. IntNurs Rev. 2014;61(1):140-7. doi: 10.1111/inr.12079.
- Reason J. Human error: models and management. BMJ. 2000;320(7237):768-70.
- Croskerry P. The importance of cognitive errors in diagnosis and strategies to minimize them. Acad Med. 2003;78(8):775-80.
- Kabirzadeh A, Bozorgi F, Motamed N, Mohseni Saravi B, Baradari A, Dehbandi M. Survey on attitude of chief managers of hospitals towards voluntary incident reporting system, mazandaran university of medical sciences, 2010-2011. J Mazandaran Univ Med Sci. 2011;21(84):131-7.
- Duthie EA. Application of human error theory in case analysis of wrong procedures. J Patient Saf. 2010;6(2):108-14. doi: 10.1097/PTS.0b013e3181de47f9.
- Biordi DL. Nursing error and caring in the workplace. NursAdm Q. 1993 Winter;17(2):38-45.
- Wilson RM, Michel P, Olsen S, Gibberd RW, Vincent C, El-Assady R, Rasslan O, Qsous S, Macharia WM, Sahel A, Whittaker S, Abdo-Ali M, Letaief M, Ahmed NA, Abdellatif A, Larizgoitia I; WHO Patient Safety EMRO/AFRO Working Group. Patient safety in developing countries: retrospective estimation of scale and nature of harm to patients in hospital. BMJ. 2012;344:e832. doi: 10.1136/bmj.e832.
- Hashemi F, shool A. One medical error and ethical response to it. Iranian Journal of Medical Ethics and History of Medicine. 2008;2(2):75-83.
- National Authorities. Iran: Islamic Penal Code [Islamic Republic of Iran]. Tehran National Legislative Bodies, April 21, 2013. Available from: http://wwwrefworldorg/docid/518a19404html.
- Asghari F, Yavari N. Statement of Medical errors. Iranian Journal of Diabet and lipid, special issue for medical ethics and history of medicine 2004;26-35.
- Kazemian M, Farshidrad S. Introduction to duties and codes in nursing profession. Forensic Medicine. 2006;12(2):108-12.
- Benner P, Sheets V, Uris P, Malloch K, Schwed K, Jamison D. Individual, practice, and system causes of errors in nursing: a taxonomy. J Nurs Adm. 2002;32(10):509-23.
- Benner P. Creating a culture of safety and improvement: a key to reducing medical error. Am J Crit Care. 2001;10(4):281-4.
- Reason J. Human error. Cambridge university press; 1990.
- Scott SD, Hirschinger LE, Cox KR, McCoig M, Brandt J, Hall LW. The natural history of recovery for the healthcare provider “second victim” after adverse patient events. QualSaf Health Care. 2009;18(5):325-30. doi:10.1136/qshc.2009.032870.
- Borhani F, Abbaszadeh A, Nakhaee N, Roshanzadeh M. The relationship between moral distress, professional stress, and intent to stay in the nursing profession. J Med Ethics Hist Med. 2014;7:3. eCollection 2014.
- Wu AW. Medical error: the second victim. The doctor who makes the mistak needs help too. BMJ. 2000;320(7237):726-7.
- Wienke A. Errors and pitfalls: briefing and accusation of medical malpractice–the second victim. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2013;12:Doc10. doi: 10.3205/cto000102.
- Dabagh A, Akbari ME, Fathi M. Medical errors in the health system. Journal of Army University of Medical Sciences(JAUMS) of the I.R.Iran; 2006.