COMMENTARY
Mandatory fortification of rice in the public distribution system in India: An ethics perspective
Jananee Muralidharan, Shalini G Hegde, Santu Ghosh, Ankita Mondal, MC Arjun, Tinku Thomas, Sunita S Kurpad, Charles Davis, Harshpal S Sachdev, Anura V Kurpad
Published online first on October 20, 2023. DOI:10.20529/IJME.2023.064Abstract
In response to the continuing high prevalence of anaemia recorded in the National Family Health Survey-5, the Indian government launched a policy for mandatory iron fortification of the rice provided through public nutrition programmes in India. This was done even though a rigorous evidence analysis had already concluded that rice fortification was not effective in preventing anaemia or iron deficiency at the population level. Fortification also poses a potential risk of iron toxicity over time, but there is no stated time period for the policy’s implementation. The risk is particularly high in segments of the population who already have a high habitual iron intake, and who could be exposed to simultaneous fortification in different staples and food commodities along with the ongoing weekly Iron and Folic Acid tablets supplementation programme. Finally, this fortification policy also requires significant additional funding and resources to implement. It is crucial to examine such mandatory health actions, and to weigh the benefits and risks of harm, using the principles of public health ethics.
Keywords: mandatory fortification, iron, public health nutrition, policy, ethics
Background
Despite ongoing targeted Iron Folic Acid (IFA) supplementation programmes, the recent National Family Health Survey-5 (NFHS-5) conducted in 2019-2021 [1] showed a higher prevalence of anaemia in India in children and women of reproductive age compared to the previous NFHS-4 conducted in 2015–2016 [2]. This increase in anaemia prevalence, despite IFA supplementation, led to a public outcry, followed by a knee-jerk launch of several initiatives, including the mandatory iron fortification of all rice in the public distribution system, to rapidly tackle this problem.
Food fortification is seen as an attractive strategy to improve the quality of diets as it is simple, has been shown to be beneficial in certain micronutrient deficiencies, and does not require significant behavioural modification by beneficiaries. In 2006, a study on iron-deficient children showed that the intake of rice fortified with micronised ferric pyrophosphate reduced anaemia prevalence [3]. However, this approach has not been uniformly successful in the context of public health, and its implementation, particularly as a mandatory intervention, needs careful deliberation.
An article published in the NITI Aayog (Public Policy Resource Centre, Government of India) portal in 2021 reflected the enthusiasm at the time for rice fortification with iron, stating: “Rice fortification…is an effective, preventive and cost-efficient complementary strategy to address the nutrition problem within a short period” [4]. Two immediate problems are apparent with this statement. First, it makes a claim about the effectiveness of fortified rice to prevent anaemia, which is not based on evidence. A robust Cochrane analysis in 2019 [5] concluded that the fortification of rice with iron alone, or in combination with other micronutrients, would make little or no difference to the risk of having anaemia or iron deficiency. Second, the duration of implementation is not stated in the policy and the criteria (or achievable target) for roll-back of the policy are omitted from the policy document.
As this fortification programme has already been rolled out, the ethical dilemmas around the imposition of mandatory fortification in public health programmes need urgent discussion.
When discussing the health of a population, as opposed to individual encounters, it is useful to consider the principles of public health ethics within existing codes and standards. The framework articulated by the Nuffield Council of Bioethics has been chosen here due to its focus on autonomy and care of the vulnerable [6]. The report lists the following components to consider: (a) proportionality, (b) scientific assessment of risk, (c) fairness and consent, (d) transparency, and (e) costs versus benefits of actions.
Proportionality
An important premise in public health ethics and policy is that the degree of interference with individual rights that public health interventions cause should be proportional to the degree of anticipated benefits. Mandatory fortification reduces the existing diversity in the cereals eaten within households, since the fortification process presumes that fortified rice will be the only cereal eaten daily, such that it can supply the claimed amount of dietary iron. Then, the intake of other cereals must decline, else the fortified rice will not be effective. The diversity of the type of rice available will also decline; rice kernels of diverse rice varieties are very varied in shape and size, but just one standard size/shape fortified rice kernel will be available, to suit perhaps only a few varieties of rice. Fortification is also likely to lead to changes in the method used to prepare rice in households. The traditional method of cooking rice in India involves first cleaning raw rice with water and then cooking it in a pot of excess water. As fortified rice kernels tend to float instead of sinking in water, the cleaning process leads to inadvertent loss of the fortified kernels, and the traditional cooking method results in only 50% of iron retention, making it the least efficient method available for cooking fortified rice [7].
Besides this interference in individual rights is the questionable benefit of fortification, based on the latest available literature. First, there is considerable uncertainty regarding the true prevalence of anaemia in India relating to the way blood is sampled and the haemoglobin (Hb) cut-off that is used to diagnose anaemia. While the NFHS [1, 2] estimates for anaemia prevalence are derived from capillary blood samples, a recent study on ~1000 women in Uttar Pradesh documented that the Hb concentration in their capillary blood was nearly 1g/dL lower than that in their venous blood, when these were measured simultaneously with the same instrument [8]. Surveys diagnosing anaemia find that prevalence based on venous blood Hb determinations is half of prevalence found when capillary blood Hb is used. This is a critical difference, as the majority have mild anaemia, and may be misclassified by the type of blood sample used for diagnosis. In a population-based study of healthy Indian children and adolescents, the 5th percentile value of their distribution of venous blood Hb was lower than the diagnostic Hb cut-off for anaemia defined by the WHO from the 5th percentile of Hb distribution in healthy White populations [9]. This furthers the position that the prevalence of anaemia in India is probably overestimated by the NFHS [9]. While contrasting viewpoints can exist in a clinical setting, where interventions can never be based on a single laboratory value, the present context relates to the Hb diagnostic level which informs public health interventions for anaemia.
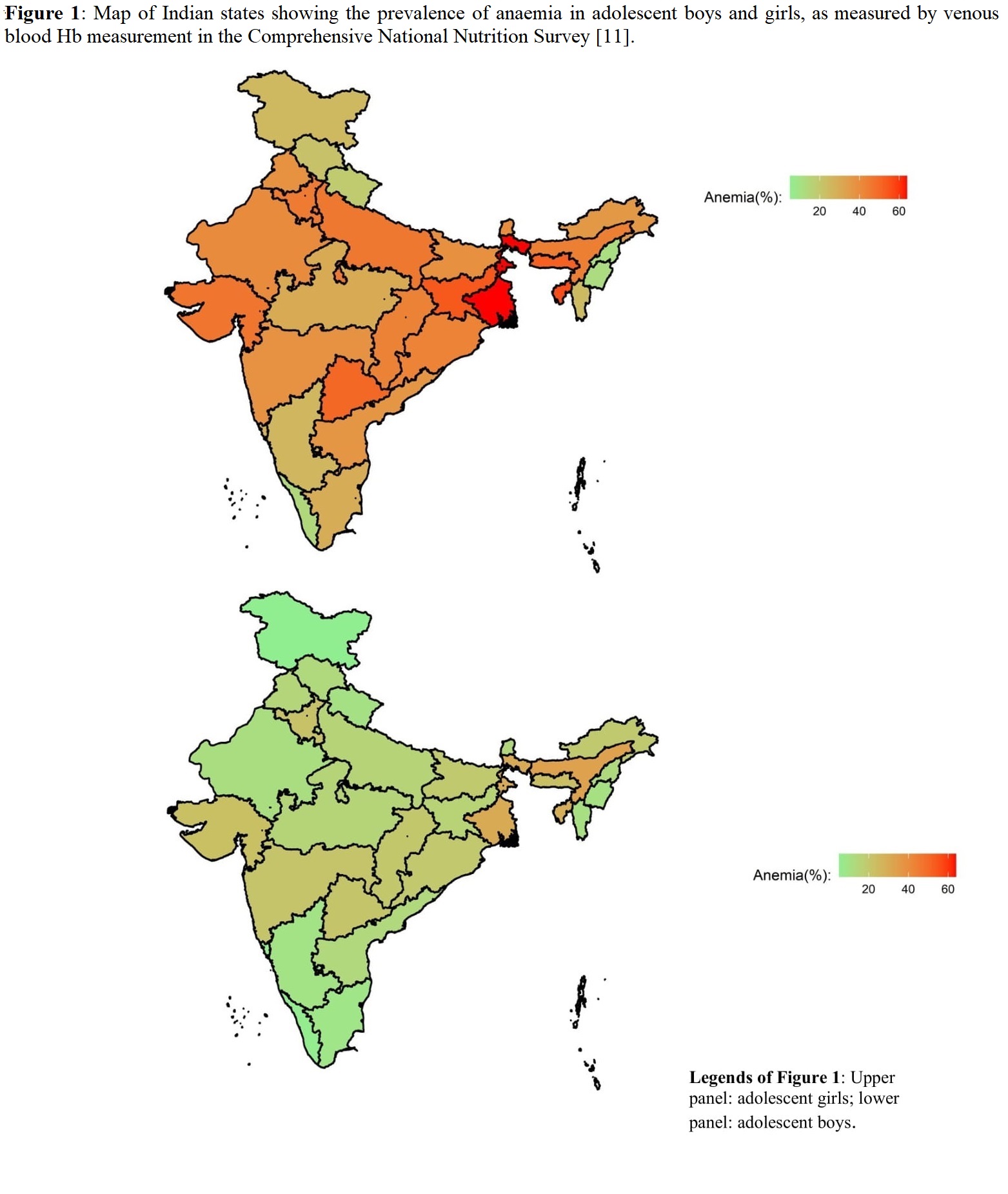
Second, iron deficiency is only one of the several causes of anaemia and contributes to 25-50% of all anaemia at different ages, in a national survey [10]. Third, as represented in Figure 1 (available online only), there is significant heterogeneity in the distribution of anaemia among male and female adolescents in each state of India (data from the Comprehensive National Nutrition Survey, CNNS [11]), implying that the one-size-fits-all approach of a mandatory universal intervention may be an inappropriate solution. Prior to imposition of a mandatory policy, it is vital to understand the true prevalence of iron deficiency and its demographic variability, and to study the impact (both beneficial and adverse) of such universal interventions among the heterogeneous population.
{kind=link}
Scientific assessment of risk
This refers to the scientific assessment of risk, including weighing of uncertainties and new evidence available on the public health intervention. The Cochrane review [5] questioned the effectiveness of rice fortification intervention globally. There is also no recent hard evidence from India which supports a mandatory policy. In the last 15 years, there have been five reported studies from India on fortified rice, with or without micronutrients. Of these, two were rigorous randomised controlled trials (RCTs) that showed no effect. An RCT from the National Institute of Nutrition, India, that provided a large amount of fortificant iron in the mid-day meal rice (19 mg iron) for eight months, found no difference in the Hb increment between the intervention and control group of children [12]. Similarly, an RCT of rice fortified with iron and other micronutrients in Bengaluru children reported no group differences in Hb concentration, anaemia, or cognitive function after six months [13].
On the other hand, three trials that showed positive effects had flaws in design, analysis, or reporting. A non-randomised, unpublished, and non-peer-reviewed study (quoted by votaries of fortification) from Gadchiroli, India, showed a minor improvement in Hb which was of no clinical significance, and was seen only when the values of mothers, girls and children were combined [14]. Another non-randomised study from Gujarat used a questionable Hb measurement method (oximeter based) [15], and a study from Kashmir had unclear statistical analyses and used a manual (without precision reportage) Hb measurement method [16].
While the fortification of foods can be a useful strategy to augment the intake of specific nutrients for addressing certain types of micronutrient deficiencies, it cannot be delivered precisely to the population in need. This is important, as many nutrients become toxic when ingested in excess and the risks should not outweigh the benefits to a section of the population. The “tolerable upper limit (TUL)” is the intake above which the risk of toxicity is unacceptable [17], and ideally, TUL should be well above the nutrient requirement value, so that even if the usual intake is higher than normal, there is no risk. However, when the TUL value of a nutrient is low, and close to the distribution of requirement values, great care must be taken when augmenting that nutrient’s intake.
The TUL for iron is quite low compared to its requirement distribution in adults. The average Indian diet already provides a median daily iron intake of 12 mg/day (interquartile range, IQR = 9-16) and 14 mg/day (IQR = 10-18) for women of reproductive age and men, respectively [18]. The Food Standards and Safety Authority of India (FSSAI) notification of the required fortification level of staple foods in India aimed to provide ~10 mg of iron/day for adults through the specified daily intake of any fortified staple food [19]. This would account for a significant portion of the daily iron requirement for Indian women and men, which is 15 and 11 mg/day respectively [17]. This is also of concern as there could be simultaneous intake of iron from different iron-fortified staple foods in the daily diet, such as rice, salt, wheat, and commercial ready-to-cook or ready-to-eat food products in India. In addition, while the FSSAI regulation for iron fortified rice presumes a fixed amount of daily rice intake (300 gm), certain states provide even higher quantities of rice in their public distribution system than other states; if the rice were fortified, that would equate to an even greater amount of iron intake. Consuming several such fortified foods can provide 20 or 30 mg/day of iron which, in addition to that naturally occurring in the diet, can clearly push intake beyond its TUL especially in groups who already have a high habitual iron intake.
Efficacy trials of fortified foods have shown that the actual fractional absorption of fortified iron is very low and ranges from 1% to 2%. The unabsorbed iron can cause adverse events like gastric irritation, nausea, and constipation, and even long-term changes downstream in the faecal microbiome [20, 21]. Even when iron is absorbed, higher storage levels (ferritin) in the body lead to increased pro-oxidative stress, linked to many chronic diseases like diabetes and hypercholesterolaemia [22, 23, 24, 25].
Individuals suffering from haematological disorders such as thalassemia major, sickle cell disease, haemochromatosis, and chronic liver disease are at risk of iron overload and the unavailability of non-fortified food options could lead to clinical deterioration. This is especially true for vulnerable indigenous communities of the country who are highly dependent on the public distribution system, but who also have high incidence of haemoglobinopathies. The prevalence of sickle cell carriers among different tribal groups in India varies from 1% to 40% and the prevalence of β-thalassemia ranges from 6% to 14% in the tribal populations of Gujarat and Odisha [26]. There is a statutory guideline to place labels on fortified food packets in India with warning messages, like: “People with thalassemia may take under medical supervision,” or “Persons with sickle cell anaemia are advised not to consume iron fortified food products”. However, the mere provision of such labels is inadequate in India, where most people who depend on the public distribution system may not be adequately literate to understand the warning or may not be consuming packaged food with a label on it, or, more importantly, may not yet be diagnosed to have an underlying haematological disease.
Moreover, the distribution of fortified rice through the public distribution system is not linked to the distribution of anaemia (Figure 1, available online only) in any given state, and hence a mismatch in demand and supply is inevitable. This illustrates the risks associated with coercive public health nutrition policies like mandatory fortification which do not consider contextual nuances.
Fairness and consent
A key concern while formulating public policy is the extent to which a government can infringe on personal liberty in the interest of population health. Depending on the gravity of the problem, governments may employ different measures ranging from the least intrusive to the most coercive. This grading of coercion within different types of public policy measures has been discussed as a policy intervention ladder [6], and a modification of this concept for the present context is depicted in a graded fashion in Figure 2.
Figure 2: The intervention ladder for policies to address iron deficiency anaemia [modified and extended from reference 6].

An example of coercive policy is to impose laws that severely restrict personal freedom to enhance public health, such as the compulsory quarantines and mandatory vaccinations during the Covid-19 pandemic to curb the spread of the virus. Here, the perceived public health benefits outweighed the curbs on individual freedom initially. However, the policy was modified repeatedly as the pandemic evolved and the severity of disease declined. In 2022, the Supreme Court of India even stated that while reasonable restrictions to prevent spread of infection can be imposed, no one can be forced to be vaccinated, citing their right to “bodily integrity and personal autonomy” [27]. While the refusal of the mandatory vaccination could pose a health risk to others, this clearly does not apply to food fortification. Policies must be weighed against anticipated risks, and must give due consideration to the autonomy of choice. This makes mandatory fortification the least ethically justified response compared to alternative policies available in Figure 2.
The dimension of social justice in mandatory single-nutrient policy actions is illustrated by the fact that iron deficiency often coexists with other micronutrient deficiencies, predominantly due to poor dietary diversity and limitations in food access. In the long term, effective measures for preventing and controlling micronutrient deficiencies require multifaceted approaches, centred on diet diversification and education to promote healthy food choices. To achieve this goal, governments must ensure that all segments of society have equitable access to diverse nutritious foods including fruits, vegetables, and animal protein. Addressing food-based strategies to overcome malnutrition is essential and must be complementary to the short-term goals of correcting micronutrient deficiencies by fortification. Indeed, focusing only on fortification erodes choices around the eating of rice varieties, and risks the reduction of any existing diversity in the cereals eaten within households. The moral legitimacy of such policies arises from the consent of those subjected to it, and it is more than likely that stakeholders, if asked, will prefer the access to simple and regular foods rather than chemically fortified foods.
In contrast to the mandatory fortification which eliminates freedom of choice for the segment of population that relies on the public distribution system, targeted IFA supplementation is the more acceptable option, but must be implemented well, through existing programmes [28]. Supplementation allows for autonomy, as targeted women can make their own decision on whether to take the IFA tablet or not, based on their personal preferences. This choice is not available for fortification: the alternative, which is unacceptable, is not to eat at all.
Transparency and accountability
An account of the evidence and reasoning behind a public health initiative demonstrates respect for the community and ensures co-operation of individuals and stakeholders. Decisions regarding fortification should not be based on other countries’ experiences, but rather on strong contextual evidence derived from local food and nutrient intake data. Independent evaluation of pilot programmes of fortified rice is necessary to assess the benefits if any. The fortification level of iron in a given food staple should be empirically derived with due consideration for population heterogeneity in iron status. In doing so, the level should be adequate to help those with deficiency, yet low enough to safeguard those with normal iron status. The programme (specifically for iron) should consider the potential risks to men, to individuals in higher socioeconomic strata accessing various sources of fortified foods, and to those with excess iron in their body due to hereditary haemolytic forms of anaemia, such as sickle cell anaemia. Moreover, it is essential to establish regulatory mechanisms to detect any adverse impact early, for example, monitoring for biomarkers of excess intake, all of which should be outlined before the programme’s rollout [29].
An example is the implementation of mandatory iodine fortification of salt, which led to a drastic reduction in iodine deficiency but also signs of excess in some populations: outbreaks of iodine-induced hyperthyroidism with excessive iodine intake have been reported in Congo [30] and Zimbabwe [31]. Furthermore, increased iodine intake can aggravate iodine-induced thyroiditis, and universal iodine fortification leaves those afflicted with this condition with no alternative sources of salt. It is imperative that the safety and well-being of the population is considered in depth, prior to the rollout of a mandatory nutritional policy.
Cost, benefits, and conflicts of interest
The conservative cost of the mandatory rice fortification policy is stated to be about Rs 2,700 crore per year [32]. This is in addition to the (considerably lower) existing cost of Rs 835 crore (based on Rs 1.09 crore cost per district) of the targeted Anaemia Mukt Bharat programme for supplemental iron (IFA) to women and children [28]. Fortification will also reflect industrial and business interests and therefore represents a potential conflict of economic and health interests in food [33]. On the other hand, a diverse healthy diet will provide multiple erythropoietic micronutrients rather than a single nutrient approach. Lastly, the technology required to manufacture rice kernels shifts the “business of supplying fortified rice” to large millers and will adversely impact smaller millers who may be unable to afford the cost of changing their technological infrastructure.
Conclusion
Mandatory fortification appears to be a utilitarian answer to a complex problem. The ethical challenges with mandatory food fortification need to be considered in their entirety, including, as stated by the WHO, “…values and preferences of the populations related to fortification of rice in different settings; trade-offs between benefits and harms; and costs and feasibility” [29]. This exercise has not been formally done in India to the best of our knowledge. An evidence-based, well-implemented targeted intervention to vulnerable groups may be a better strategy to combat anaemia in comparison to mandatory food fortification. It is essential to ensure that policies promote well-being, and are fair, respectful of individual autonomy, cost-effective and free from potential harm.
*Joint First Authors: JM and SGH
Disclosure of Conflict of Interest: HSS was a member of the Scientific Panel for Food Fortification and Nutrition and Scientific Committee of the Food Safety and Standards Authority of India (FSSAI). AVK was a member of the Scientific Committee of FSSAI.
Acknowledgement: None
Funding Support: None
References
- Ministry of Health and Family Welfare, Govt of India. National Family Health Survey, India. NFHS-5. 2019-20. New Delhi: MoHFW; 2021[Cited 2023 Apr 3]. Available from: http://rchiips.org/nfhs/nfhs5.shtml
- Ministry of Health and Family Welfare, Govt of India. National Family Health Survey, India. NFHS-4. 2015-16. New Delhi: MoHFW; 2017 Dec [Cited 2023 Apr 3]. Available from: http://rchiips.org/nfhs/nfhs4.shtml
- Moretti D, Zimmermann MB, Muthayya S, Thankachan P, Lee TC, Kurpad AV, Hurrell RF. Extruded rice fortified with micronized ground ferric pyrophosphate reduces iron deficiency in Indian schoolchildren: a double-blind randomized controlled trial. Am J Clin Nutr. 2006; 84:822-9. https://doi.org/10.1093/ajcn/84.4.822
- Kumar R, Shekhar V. Rice fortification is an effective way to combat anaemia. NITI AYOG. 2021 Oct 28[Cited 2023 Apr 3]. Available from: https://www.niti.gov.in/rice-fortification-effective-way-combat-anemia.
- Peña-Rosas JP, Mithra P, Unnikrishnan B et al. Fortification of rice with vitamins and minerals for addressing micronutrient malnutrition. Cochrane Database Syst Rev. 2019 Oct 25;2019(10):CD009902. https://doi.org/10.1002/14651858.cd009902.pub2
- Nuffield Council on Bioethics. Public health: ethical issues. London, United Kingdom: Nuffield Council on Bioethics; 2007[Cited 2023 Apr 3]. Available from: https://www.nuffieldbioethics.org/publications/public-health.
- Losso JN, Karki N, Muyonga J, Wu Y, Fusilier K, Jacob G, et al. Iron retention in iron-fortified rice and use of iron-fortified rice to treat women with iron deficiency: A pilot study. BBA Clin. 2017 Sep 8; 8:78-83. https://doi.org/10.1016/j.bbacli.2017.09.001
- Neufeld LM, Larson LM, Kurpad A, Mburu S, Martorell R, Brown KH. Hemoglobin concentration and anemia diagnosis in venous and capillary blood: biological basis and policy implications. Ann N Y Acad Sci. 2019 Aug;1450(1):172–189. https://doi.org/10.1111/nyas.14139
- Sachdev HS, Porwal A, Acharya R, Ashraf S, Ramesh S, Khan N, et al. Haemoglobin thresholds to define anaemia in a national sample of healthy children and adolescents aged 1-19 years in India: a population-based study. Lancet Glob Health. 2021 Jun [Cited 2023 Apr 3];9(6):e822–e831. Available from: https://www.thelancet.com/pdfs/journals/langlo/PIIS2214-109X(21)00077-2.pdf
- Sarna A, Porwal A, Ramesh S, Agrawal PK, Acharya R, Johnstone R, et al. Characterisation of the types of anaemia prevalent among children and adolescents aged 1-19 years in India: a population-based study. Lancet Child Adolesc Health. 2020 Jul;4(7):515¬–525. https://doi.org/10.1016/s2352-4642(20)30094-8
- Ministry of Health and Family Welfare, Government of India, UNICEF, Population Council. Comprehensive National Nutrition Survey 2016–2018. National Health Mission; 2019[Cited 2023 Apr 3]. Available from: https://nhm.gov.in/showfile.php?lid=712
- Radhika MS, Nair KM, Kumar RH et al. Micronized ferric pyrophosphate supplied through extruded rice kernels improves body iron stores in children: a double‐blind, randomized, placebo‐controlled midday meal feeding trial in Indian schoolchildren. Am J Clin Nutr. 2011;94:1202‐1210. https://10.3945/ajcn.110.007179
- Thankachan P, Rah JH, Thomas T et al. Multiple micronutrient-fortified rice affects physical performance and plasma vitamin B-12 and homocysteine concentrations of Indian school children. J Nutr. 2012;142:846–52. https://doi.org/10.3945/jn.111.149021
- IIHMR University, Tata Trusts. Impact Assessment of Rice Fortification Pilot Study in Gadchiroli, Maharashtra. [Cited 2023 Apr 3]. Available from: https://ffrc.fssai.gov.in/assets/event/file/impact-assesment-of-rice-fortification-dr-dk.pdf” https://ffrc.fssai.gov.in/assets/event/file/impact-assesment-of-rice-fortification-dr-dk.pdf.
- Mahapatra S, Parker ME, Dave N et al. Micronutrient-fortified rice improves haemoglobin, anaemia prevalence and cognitive performance among schoolchildren in Gujarat, India: a case-control study. Int J Food Sci Nutr. 2021;72:690¬–703. https://doi.org/10.1080/09637486.2020.1855126
- Hussain SZ, Singh B, Rather AH. Efficacy of micronutrient fortified extruded rice in improving the iron and vitamin A status in Indian schoolchildren. Int J Agri Food Sci Tech. 2014;5:227‐38. Available from: https://www.ripublication.com/ijafst_spl/ijafstv5n3spl_16.pdf
- Indian Council of Medical Research / National Institute of Nutrition. Nutrient Requirements for Indians. A report of the expert group. Department of Health Research, Ministry of Health and Family Welfare, Government of India. 2020. [Cited 2023 Apr 3]. Available from https://www.nin.res.in/rdabook/brief_note.pdf
- Ghosh S, Thomas T, Pullakhandam R, Nair KM, Sachdev HS, Kurpad AV. A proposed method for defining the required fortification level of micronutrients in foods: An example using iron. Eur J Clin Nutr. 2022 Sep 8. https://doi.org/10.1038/s41430-022-01204-4
- The Gazette of India: Extraordinary. Part II – Section 4. Food Safety and Standards (Fortification of Foods) Regulations 2018. Notification. Government of India, 2018. [Cited 2023 Apr 3]. Available from: https://www.fssai.gov.in/upload/uploadfiles/files/Compendium_Food_Fortification_Regulations_30_09_2021.pdf
- Tolkien Z, Stecher L, Mander AP, Pereira DI, Powell JJ. Ferrous sulfate supplementation causes significant gastrointestinal side-effects in adults: a systematic review and meta-analysis. PloS One. 2015 Feb 20;10(2):e0117383. https://doi.org/10.1371/journal.pone.0117383
- Jaeggi T, Kortman GAM, Moretti D, Chassard C, Holding P, Dostal A, et al. Iron fortification adversely affects the gut microbiome, increases pathogen abundance and induces intestinal inflammation in Kenyan infants. Gut. 2015 May; 64:731–42. https://doi.org/10.1136/gutjnl-2014-307720
- Simcox JA, McClain DA. Iron and diabetes risk. Cell Metab.2013 Mar 5; 17(3):329-341. https://doi.org/10.1016/j.cmet.2013.02.007
- Jiang L, Wang K, Lo K, et al. Sex-Specific Association of Circulating Ferritin Level and Risk of Type 2 Diabetes: A Dose-Response Meta-Analysis of Prospective Studies. J Clin Endocrinol Metab. 2019 Oct 1;104(10):4539–4551. https://doi.org/10.1210/jc.2019-00495
- Kim YE, Kim DH, Roh YK, et al. Relationship between serum ferritin levels and dyslipidemia in Korean adolescents. PLoS One. 2016 Apr 12;11(4): e0153167. https://doi.org/10.1371/journal.pone.0153167
- Kim MK, Baek KH, Song K-H, et al. Increased serum ferritin predicts the development of hypertension among middle-aged men. Am J Hypertens. 2012 Apr; 25(4):492–497. https://doi.org/10.1038/ajh.2011.241
- Teli AB, Deori R, Saikia SP. Haemoglobinopathies and β-thalassaemia among the tribals working in the tea gardens of Assam, India. J Clin Diagn Res: JCDR. 2016;10(12):LC19. https://doi.org/10.7860/jcdr/2016/22010.9002
- Supreme Court of India. Jacob Puliyel v Union of India and Ors. Writ Petition (Civil) No. 607 of 2021. 2022 May 2[Cited 2023 May 29]. Available from: https://main.sci.gov.in/supremecourt/2021/12077/12077_2021_5_1502_35439_Judgement_02-May-2022.pdf
- Anaemia Mukt Bharat. Budget factsheet. FY 2019–20 and FY 2020–21 [Internet]. New Delhi, India: National Health Mission, Government of India; 2021. [Cited 2023 Apr 3]Available from: https://anemiamuktbharat.info/wp-content/uploads/2021/01/AMB-Budget-Factsheet-18-01-2021.pdf.
- WHO. Guideline: fortification of rice with vitamins and minerals as a public health strategy. Geneva. 2018. [Cited 2023 Apr 3]Available from: https://www.who.int/publications/i/item/9789241550291
- Bourdoux PP, Ermans AM, Mukalay wa Mukalay A, Filetti S, Vigneri R. Iodine-induced thyrotoxicosis in Kivu, Zaire. Lancet. 1996;347:552-553. https://doi.org/10.1016/s0140-6736(96)91188-5
- Todd CH, Allain T, Gomo ZA, Hasler JA, Ndiweni M, Oken E. Increase in thyrotoxicosis associated with iodine supplements in Zimbabwe. Lancet. 1995;346:1563-1564. https://doi.org/10.1016/s0140-6736(95)92095-1
- Cabinet Committee on Economic Affairs (CCEA). 2022. [Cited 2023 Apr 3]Available from: https://pib.gov.in/PressReleasePage.aspx?PRID=1814826.
- Lawrence M. Food fortification: the evidence, ethics, and politics of adding nutrients to food. Oxford University Press; 2013 Jan 3. https://doi.org/10.1093/acprof:oso/9780199691975.001.0001