INTERNATIONAL ETHICS
Informed consent in an antiretroviral trial in Nigeria
Ogenna Manafa, Graham Lindegger, Carel Ijsselmuiden
DOI: https://doi.org/10.20529/IJME.2007.009
Abstract
We examined the process of informed consent in an antiretroviral trial in Nigeria. A semi-structured questionnaire was administered to 88 out of 180 people enrolled in the trial. This covered all aspects of the information disclosed in the leaflet of the antiretroviral trial. We found that 75 (85 per cent) of the respondents knew that the purpose of the research was to test a new drug and 13 (14 per cent) believed that they were receiving free treatment for HIV. Participants understood certain aspects of the research, especially the benefits and duration. Their understanding of the trial’s risks and their right to refuse to participate and to withdraw was low. Their level of understanding was significantly related to age but not to gender, marriage, education, religion, employment and occupation.
Signed informed consent is not a guarantee that participants have understood the information given to them and therefore made a voluntary decision to participate. Researchers should make sure that the process of obtaining informed consent achieves the desired outcome. This is especially important in the developing world where access to health care is limited, potential participants are poor and literacy levels are low.
Introduction
The emphasis on a person’s right to accept or refuse to participate in biomedical research reflects important ethical principles such as respect for human dignity and autonomy. Informed consent for research on humans usually incorporates five essential components: a) the capacity to consent, b) disclosure of all relevant information about the research, c) the prospective participants’ comprehension of this information for making an informed decision, d) the prospective participants’ freedom from all coercion, and e) explicit and formal consent by the participant, usually in writing (1, 2).
Informed consent is complex. It is one thing to get potential participants to sign a form indicating that they have been informed about a trial, but another to achieve a participant’s understanding. To make the decision, the participant has to fully understand the information provided. As Faden and Beauchamp (3) have suggested, this involves three stages: a) the transmission and reception of information, b) the comprehension of information, and c) the use of information in arriving at a decision.
The goal of the process of informed consent is to make sure that research participants achieve informed decisions and then implement them. But the interaction between the researchers and participants is nearly as important as the outcome of their discussions. The issue of informed consent therefore implies a sharing of information.
In some cultures, the belief system of potential research participants does not use the concepts and terms of modern medical science and technology to explain health and disease. Studies have provided examples of pervasive beliefs about diseases and causes of death such as sorcery, spirits and forbidden food. This is significant, because when people do not understand or accept scientific explanations of health and disease, the challenge of obtaining informed consent can be daunting (4). Are we really gaining informed consent from people who may not believe in the germ theory of disease?
More research is needed in the process of obtaining informed consent and whether participants actually understand the information given to them. We examined the process of informed consent in a group of clinical trial participants to assess their understanding of the study in which they were participating, and the relationship of their understanding with demographic characteristics such as age, gender and education.
Methodology and analyses
The study aims to assess the adequacy of understanding of the information by study participants.
The study involved participants enrolled in a clinical trial of an antiretroviral therapy (ART) in Nigeria. The ART clinical trial is a non-inferiority trial involving a new (generic) antiretroviral drug to be marketed within the country and a drug already approved and used in the treatment of HIV. At the time of the study, ART was available in some pharmacies in major cities of the country, but it cost US$200 for a complete course for a month and US$100 for a generic, which is beyond the reach of most HIV positive individuals in Nigeria. HIV patients in the country at the time of the study were mainly treated through five federal government centres that provided ART at a subsidised rate of US$10 per month. The patient information sheet and informed consent form for the ART trial indicated that it was a research study and explained the purpose of the research.
All 180 people enrolled in the clinical trial were invited to participate; 70 initially agreed and 18 more volunteered later. The 88 participants comprised 48.8 per cent of the persons enrolled in the study. Data were collected through a questionnaire.
The information leaflet given to participants in the ART trial was used to design the questionnaire. The questionnaire used both structured and unstructured questions. Some of the questions had an open format; this enabled us to assess the participants’ comprehension of technical information. These questions asked for explanations and could be answered in a variety of ways. The questionnaire was pre-tested on a sub-sample similar to our target sample. The researcher, together with a trained interviewer, administered the questionnaire. The questionnaire was administered to all 88 participants two months after they were enrolled in the ART trial.
The questions covered knowledge of four main categories: the aims of the research and eligibility of participants, the risks and benefits, the right to refuse participation and withdraw from participation, and the practical procedures of the research. The maximum scores were 4, 10, 4 and 7 respectively for the four categories, and the overall knowledge score was 25. Responses were evaluated and recorded as either right or wrong. Scoring was based on information given to the participants about the trial.
A mean knowledge score of the four categories was obtained. The following cut-offs were used: a score of 75 per cent meant excellent knowledge, 60-74 per cent was good knowledge, 50-59 per cent meant moderate knowledge, 30-49 per cent was poor knowledge, and 0-29 per cent meant extremely poor knowledge.
After scoring, the data were entered in a computer database and analysed with STATA software. Percentages of fully correct, partially correct and incorrect answers were used to evaluate the subjects’ understanding. Frequency distribution was generated for all variables and later for collapsed categories. A spearman rank correlation, student’s T-test and one-way ANOVA were done to test the relationship between understanding and the demographic variables of education, gender and socio-economic status.
Results and discussion
Of the 88 respondents, 51 were female and 39 were male. The mean age of the participants was 39.2 (range 26-62). The majority (73) were Christian and 55 were married at the time of the study (Table 1). Sixty-six were employed at the time of study with a high percentage of civil servants and people doing business. All the respondents had some education and 22 were university graduates.
The majority of the respondents (75) knew they were enrolled to participate in research and 13 thought they were involved in a treatment schedule. Fifty-seven participants reported that doctors explained the trial; the counsellors explained the research to 23 of the participants, and nurses explained it to eight participants.
| Table 1. Demographic characteristics of respondents | |||
| Demographic characteristics | No | % | |
| Sex | Male
Female |
51
37 |
57.9
42.1 |
| Employed | Yes
No |
66
22 |
75
25 |
| Married | Yes
No |
55
33 |
62.5
37.5 |
| Religion | Christian
Islam |
73
15 |
82.9
17.1 |
| Education | Primary
Secondary College/Technical University graduate Beyond first degree |
12
33 19 22 2 |
13.6
37.5 21.6 25 2.3 |
When asked if they knew why they were invited to participate in the study, 63 respondents said yes. Various reasons were mentioned, but 57 of those who responded in the affirmative knew it was because of their HIV status. Almost half (43) knew the drug given acted to reduce viral loads. The other major use of drug mentioned was to sustain and live a healthy life (21). The mean knowledge for the respondents was 1.72 (range 1-4) with a standard deviation (SD) of 0.840
All the respondents knew of at least one benefit of the study. Most of the benefits mentioned related to cost; 61 mentioned free tests and check ups. The risks of the research were poorly understood. Only 23 knew that risks were involved in participating in the study. One participant who said he was aware of risks could not mention any. A diminishing of the immune system, general side effects of the drugs, death on discontinuation, inefficacy of the drug, and compliance issues were some of the perceived risks mentioned by participants. The respondents’ mean score was 2.9 (range 1-10, SD 1.9).
Only 18 respondents indicated that not all study participants were receiving the same drug. Ten of these 18 did not know what the others were receiving and three respondents claimed that they were not told about participants receiving different drugs. The rest said they did not care what the others were receiving because receiving a good drug was the important thing.
| Table 2. Mean understanding of the information by respondents | ||||
| Knowledge type | Maximum score | Mean score | Range | STD.
DEV |
| Aim and eligibility | 4 | 1.72 | 1 – 4 | 0.840 |
| Methods and RTFW | 10 | 4.92 | 1 – 4 | 1.942 |
| Second table column entry | 4 | 1.49 | 1 – 10 | 1.406 |
| Practical procedures | 7 | 3.45 | 1 – 8 | 1.50 |
| Overall knowledge | 25 | 10.625 | 1 – 25 | 3.343 |
| Table 3. Benefits of research as mentioned by respondents | ||
| Benefits | No | % |
| Free tests and check ups | 61 | 69.3 |
| Receive new drug at a cheaper rate | 25 | 28.4 |
| Get another drug if the one am currently on is not working | 17 | 19.3 |
| Feel better from illness | 15 | 17 |
| Monitored at no cost | 14 | 15.9 |
| More knowledge and ideas | 10 | 11.4 |
| Be first to receive new drug | 9 | 10.2 |
| Peaceful heart/ relief | 9 | 10.2 |
| Table 4. Understanding of practical procedures in the trial | ||
| What participation involves | No | % |
| Do thorough examinations | 66 | 75 |
| Draw blood | 47 | 53.4 |
| Adhere to drug strictly | 5 | 5.7 |
| Receive new drug | 30 | 34.1 |
| Get counselling | 21 | 23.9 |
| Maintain a good diet | 10 | 13.4 |
| Attend to my complaints | 9 | 10.2 |
Eighteen respondents believed that they could not refuse to participate in the research at the time of recruitment, while six did not know about their right to refuse. A higher number believed they could withdraw from the research after they had agreed to participate, and 64 and 58 knew they could withdraw or refuse, respectively.
When asked what would happen if they decided to withdraw, 23 said they would lose their benefits. That is, they would be withdrawn from the trial drug. The other consequences of withdrawal that were mentioned were: reverting back to initial status (14), being seen as ungrateful (12), and it being unwise to withdraw when still HIV positive (11). The mean knowledge score of respondents for this category was 1.48 (range 1-4, SD 1.41) (Table2).
A total of 74 respondents understood what procedures their participation in the trial involved. Sixty-six mentioned more than one procedure, and 68 knew how many visits a year were expected of them and at what intervals. Seventeen of these did not know how long the research would last. The mean understanding of respondents in this category was 3.45 (range 1-7, SD 1.50).
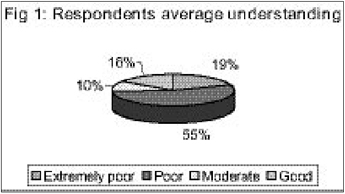
The maximum score for understanding was 25. The mean participants’ understanding was 10.625 (range 1-25, SD 3.34). None of the respondents had an understanding that could be described as "excellent", and the majority were in the "poor understanding" category.
The overall findings suggest that the respondents’ understanding of their participation in the trial was poor and inadequate. They seemed to best understand the benefits and eligibility for the study, and least understand the risks and research methods. This strongly indicated that participants did not adequately understand the information given to them or that adequate information was not provided.
The study tested the hypothesis that the level of understanding was related to the demographic characteristics of the respondents. Statistical analysis using the spearman rank correlation showed that there is an inverse relationship between understanding and age, with persons below 40 having a better understanding (p= 0.003) (Table 5). The younger age group also had better and more comprehensive education.
Analysis using the students t test showed that no association exists between understanding and sex (p= 0.617), understanding and marital status (p= 0.590), understanding and education (p= 0.112), and understanding and employment (p= 0.674). The one-way analysis of variance showed that there was no association between understanding and religion (p=0.667, f= 0.03).
Discussion
The Declaration of Helsinki (2) and the guidelines of the Council for International Organization of Medical Sciences (5) both state that prospective participants in research must understand the information given to them before they can make an informed decision to consent. Questions have been raised about the participants’ understanding of information, especially in Africa and other parts of the developing world, where literacy is low and concepts of disease and illness vary.
| Table 5. Relationship between understanding and age of respondents | |||||
| Understanding | Age <=30 | Age
31- 40 |
Age
40 – 50 |
Age >50 | Total |
| No (%) | No (%) | No (%) | No (%) | No (%) | |
| Extremely poor | 8 (44.4) | 5 (13.2) | 3 (15.8) | 1 (7.8) | 17 (19.3) |
| Poor | 4 (22.2) | 27 (71.1) | 10 (52.6) | 7 (53.8) | 48 (54.6) |
| Moderate | 2 (11.1) | 2 (5.3) | 4 (21.1) | 1 (7.8) | 9 (10.2) |
| Good | 4 (22.2) | 4 (10.5) | 2 (10.5) | 4 (30.8) | 14 (15.9) |
| Total | 18 (20.5) | 38 (43.2) | 19 (21.6) | 13 (14.8) | 88 (100) |
The risk of therapeutic misconception has been widely reviewed and reported (6, 7, 8). The results of our study show that while a majority of the participants knew that this was a trial, some of them thought that this was a treatment regime. In fact, a small number of participants strongly expressed their conviction about the therapeutic efficacy of the treatment, despite the information provided.
The participants had a better overall knowledge of the benefits of the research than the risks. The majority could mention one correct benefit, but a large percentage did not even know that risks were involved in participating. Some who claimed to know of the risks could not remember any.
We did not observe the consent process because all the respondents had enrolled in the research two months before the interview, but we did observe the process that was underway at the time of our interviews. In most cases the research team focused on the benefits of participation in the trial and the need to comply with the treatment protocol. They seemed to avoid discussing potentially controversial or complicated issues. The risks were explicitly explained in the information leaflet, but participants appeared to have little or no understanding of these risks. There could be many reasons for the researchers’ inadequate disclosure of risks, such as cultural sensitivity, exploitation of the participants, and inadequate understanding of what a consent process involves. A lack of understanding of the risks in research means that trial participants cannot properly weigh the benefits and risks to make an informed choice.
A large percentage of participants knew about their right to withdraw, but many saw withdrawing as being "disrespectful" or leading to a loss of benefits. They were not aware that withdrawing from the trial would not have any negative implications. Their right to withdraw without any subsequent consequences may not have been properly explained or participants may not have comprehended this information.
The respondents’ average understanding of the practical procedures of the research was the highest of the knowledge categories. Most of them mentioned one important procedure that the trial entailed. This might be due to the fact that people are sensitive to blood being drawn from them for a test. Another explanation could be the controversy concerning their tests and results.
Despite the fact that blood would be drawn from them to test their viral load, respondents were told that they would not get a copy of the test results. They believed this was a disadvantage. Most of the participants understood that it is only through drawing of blood and doing the necessary tests that the effect of the drug on their viral load could be documented.
The overall level of understanding was low probably because the informed consent was a one-off process or because participants assumed the research was a way to improve their quality of life and were not particular about the details. They did not have a copy of the information form and could not read or have the information read to them again. When a clinical trial involves first-time participants, it is important to put time and effort in giving them information and making sure that the information is understood.
Conclusions
The principal aim of this study was to ascertain how well participants in clinical trials understood the information given to them during the process of informed consent. The participants did not understand some of the major information provided in the consent leaflet. Since we did not examine the consent process of those we interviewed, we do not know if this was because the information was not adequately provided.
A signed consent is not a guarantee that patients have actually understood what they have signed. A completed consent form implies only that the research team has completed the process of formal informed consent. It does not necessarily guarantee that they have fulfilled their ethical responsibilities. Faden and Beauchamp (3) have argued that the practice of informed consent is driven by a legal as well as an ethical agenda. The legal agenda is strongly influenced by litigation and is based on a defensive medical approach. The ethical or moral agenda is driven by the idea that research participants are autonomous agents and have a right to determine what will happen to them. It sees informed consent as a process of shared decision-making.
Effective communication depends on the interaction between the research team and the participants. Researchers must always determine whether their efforts at informed consent achieve the desired outcome of the participants’ understanding. This is particularly important in developing countries where the level of education is low, and participants are often economically deprived and at a lower social status than the researchers.
References
- The Nuremberg Code. [cited 2005 Oct 10]. Available from the website of the United State Holocaust Memorial Museum http://www.ushmm.org/research/doctors/codeptx.htm
- World Medical Association. Declaration of Helsinki. Ethical principles for medical research involving human subjects; 2000. [cited 2005 Oct. 10]. Available from the WMA website www.wma.net/e/policy/b3.htm
- Faden R, Beauchamp T. A history and theory of informed consent. 1st ed. New York: Oxford University Press; 1986.
- National Bioethics Advisory Commission (NBAC). Ethical and policy issues in international research: clinical trials in developing countries. Report and recommendations of the NBAC. Bethesda, Maryland; 2001 [cited 2005 Oct. 12]. Available from: www.georgetown.edu/research/nrcbl/nbac/pubs.htm
- Council for International Organization of Medical Sciences (CIOMS). International ethical guidelines for biomedical research involving human subjects. Geneva: World Health Organisation; 2002 [cited 2005 Oct 12]. Available from: http://www.cioms.ch/frame_guidelines_nov_2002.htm
- Appelbaum P, Roth LH, Lidz C. The therapeutic misconception: informed consent in psychiatric research. Int J Law Psychiatry 1982; 5 (3-4): 319-29.
- Roth L, Lidz CW, Meisel A, Soloff PH, Kaufman K, Spiker DG, Foster FG. Competency to decide about treatment or research: an overview of some empirical data. Int J Law Psychiatry 1982; 5: 29-50. 8.
- Appelbaum P, Roth LH, Lidz, CW, Benson P, Winslade W. False hopes and best data: consent to research and the therapeutic misconception. Hasting Cent Rep 1987 April; 17(2): 20-4.