RESEARCH ARTICLE
Human dignity of patients in nursing: A concept analysis
Vahid Zamanzadeh, Nasib Babaei, Leila Valizadeh, Marziyeh Avazeh
Published online first on September 2, 2022. DOI:10.20529/IJME.2022.066Abstract
To understand the concept of dignity in care and use it in practice, nurses need a clear understanding of the dignity of patients, which can help them improve quality of care and provide services of a higher standard. This study aims to clarify the concept of human dignity of patients in nursing. Walker and Avant’s method (2011) was used for this concept analysis. Published literature from 2010 to 2020 was identified using national and international databases. The full text of the included articles was reviewed. The main dimensions and attributes include valuing the patient, respecting patients’ privacy, autonomy, and confidentiality, having a positive mental image, having a sense of altruism, respecting human equality, observing patients’ beliefs and rights, adequately educating patients, and paying attention to secondary caregivers. Nurses should consider the subjective and objective aspects of dignity in their daily care activities by cultivating a deeper understanding of the concept of dignity and its attributes. In this regard, nursing tutors, managers, and policymakers in healthcare should emphasise human dignity in nursing.
Keywords: concept analysis, human dignity, patient, nursing
Introduction
The concept of dignity has a long history spanning from prehistoric times to the advent of modern ethical and legal discourses. Traditional concepts such as Imago Dei (Image of God), wisdom, freedom, natural law, and conscience are based on interpretations of dignity [1]. Various religions and philosophers throughout history have provided diverse interpretations of the concept. In the twentieth century, the Universal Declaration of Human Rights was the first document to integrate the concept of human dignity in a global legal framework. The Declaration states that all human beings are born free and with equal dignity and rights [2]. The term “dignity” is defined as entailing respect and self-worth and overlaps with concepts such as hope, self-exaltation, self-confidence, quality of life, and self-respect [3].
Dignity is a subjective concept that is interpreted differently by individuals and cultures [4]. It can be classified into “absolute dignity” and “relative dignity”. The former is a universal value and is based on human rights. All human beings are valuable because they are human, regardless of their situation and condition [5]. Maintaining the dignity of patients in healthcare systems is important [6]. Absolute dignity is the same for all human beings and does not change, while relative dignity can change and is influenced by culture, society, and education [5, 7]. Thus, in recent decades, much attention has been paid to exploring the nature of human dignity and its relationship to healthcare practices [8, 9, 10, 11, 12].
Preserving a patient’s dignity and value and respecting their human rights are critical to nursing [13, 14] and are specified in nursing ethics codes [15]. Nevertheless, patients are still at risk of losing their dignity [16] at the hands of the nursing staff, which may influence the provision of respectful care [16, 17]. Several studies indicate that dignity is not respected in care settings. A lack of respect for human dignity is associated with negative feelings such as fear, disbelief, shock and denial, anger, hatred, apathy, sadness, and frustration and ultimately has undeniable effects on patients’ health [18, 19].
To understand dignity in care and use the concept in practice, nurses need a clearer understanding of dignity and how to provide services with dignity [20]. There has been no consensus on the characteristics of dignified care, whether in general [21, 22] or in terms of specific aspects [23, 24]. Therefore, understanding patient dignity requires an understanding of the cultural context, the unique characteristics of diverse countries, and the common perception of human dignity across the international human community [25].
Considering the difficulties associated with understanding the nature of human dignity in nursing and clinical practice and building a global consensus on the concept, there is still no clear definition of the concept [26]. However, according to some studies in Iran, factors such as treating patients with empathy, creating a relaxed physical environment, respecting patients’ privacy, beliefs, and values, ensuring patients’ participation in decision-making, providing impartial care, improving patients’ awareness of treatment methods, and providing psychosocial support help maintain patient dignity in hospital settings [11, 27, 28, 29, 30]. Further, since respect for human dignity and providing ethical care are among the most important needs of patients [10], the use of appropriate and easy-to-understand language while providing care services requires particular attention, especially among nurses [19]. Despite the recent attention the concept of dignity has received, it remains complex and ambiguous, and there is no comprehensive and specific definition that has been agreed upon by experts [31, 32, 33].
So, it seems necessary to develop nurses’ insight and knowledge about maintaining patients’ dignity and the factors affecting it [34]. To upgrade standards of care and improve the quality of services provided, and to make nurses and nursing students more aware of the dignity of patients in their daily care activities, they must first be familiarised with the concept of dignity and its various aspects. Additionally, the views of patients should be clarified. Since there is ambiguity in the definition of dignity, and nurses do not have a clear understanding of it, the present study was conducted to delineate the concept of dignity and determine its dimensions in order to enhance the dignity of patients and clients.
Methods
The study was conducted in 2020, using the basic principles of the Walker and Avant concept analysis approach [35] to clarify and determine the specifics and characteristics of patients’ human dignity in nursing. The Walker and Avant concept analysis method is a linguistic and practical approach used to analyse explicit and implicit definitions of a concept in order to determine its characteristics, antecedents, and consequences in practice and research [35]. This framework was used because of its step-by-step and user-friendly approach. The method was taken from Wilson (1963) and initially consisted of 11 steps but was simplified into eight steps: 1) selecting a concept; 2) determining the purpose; 3) identifying all uses of the concept; 4) determining the defining attributes; 5) presenting a model case; 6) constructing additional cases; 7) clarifying antecedents and consequences; and 8) defining empirical referents [35]. A comprehensive review of the literature was carried out using national databases — MagIran, SID, IranMedex, and IranDoc, and international databases — CINHAL, PubMed, Scopus, ProQuest, Science Direct, Google Scholar, and Ovid. The keywords used were “human dignity”, “patient dignity”, “dignity*”, “promoting dignity”, “dignity of the human being”, “dignity-related factors”, “dignity in care”, “privacy”, and “respect” and a combination of the keywords “dignity*”, “care”, “privacy”, “respect”, “dignity of the human being”. After searching databases, a number of reputable journals were reviewed manually (hand searching). In addition, the references (references of references) of selected articles were searched. In collecting the available literature, the comprehensive search was limited to research studies published between 2010 and 2020. Articles published between 2010 and 2020, pertinent to human dignity in nursing or related issues, focused on Iran, published in Persian and English, and for which the full text was available were included. The exclusion criteria were papers presented at conferences and seminars, educational papers, papers published in invalid journals [Invalid journals (blacklisted) are known in the source finder system of the Ministry of Health of Iran], and letters to the editor. The extracted information was analysed using the Walker and Avant concept analysis approach. EndNote x7 reference management software was used to organise articles, study the titles and abstracts, and identify duplicates.
Results
All articles containing definitions, characteristics, classifications, and consequences of human dignity were included in the study. In total, 47 articles and one dissertation (48 studies) were found, and 27 of them were omitted for not meeting the inclusion criteria. Finally, 21 related studies were reviewed.
Selecting a conceptA concept is considered important when it is widely used, emphasised, studied, and surveyed. Further, a concept can be clarified through in-depth analysis [35]. Human dignity is an important concept for health professionals. Respecting and cherishing the existential dignity of individuals is the foundation of nursing practice, medicine, and nursing care. Dignity is also a fundamental principle and ensuring it is considered a duty in national and international nursing and medicine ethical codes [32]. However, the concept, regardless of its increasing use as a tool to promote respect for human value in political, social, and legal arrangements, lacks an obvious and explicit definition [36]. Further, there is still insufficient information on how to treat patients with respect [31]. Additionally, a clear and accepted definition of human dignity within nursing is lacking. Thus, clarifying this concept by identifying the different dimensions of dignity can help us upgrade standard of care and improve the quality of service by creating opportunities to provide services while preserving the dignity of patients in a clinical setting.
Determining the purpose of analysisThe purpose of this analysis is to use the Walker and Avant approach to explore the concept of human dignity of patients in nursing. We examine the internal structures of this vague concept, identify its components, and clarify its meaning [35]. By decreasing its ambiguity, the findings help to increase consistency in the application of this concept and determine the meaning of dignity in nursing care.
Identifying all uses of the conceptIdentifying the applications of the concept enables a richer understanding of it and validation of defined features [35]. Importance, status, and human dignity are terms that have long been used in Islamic religious texts. From the point of view of the Quran, all human beings are worthy of respect and have inherent status and dignity. This issue has been emphasised in different chapters of the Quran [37]. In the nurses’ moral workbook, a philosophical definition is used that highlights the inseparable and unique part of a person. In fact, the philosophical aspect is related to the unique value of individuals [38]. Dignity can be understood as resulting from the interaction of capabilities and environmental conditions — that is, when people are in an unfavourable condition and they feel incompetent and vulnerable, their sense of status and dignity decreases [39]. Borhani et al present a new understanding of patient dignity in Iran by categorising it into fundamental dignity and transcendent dignity — fundamental dignity helps to achieve physical and mental health and should be observed for all patients, while transcendent dignity is equal to physical, social, mental, and spiritual health. In fact, the goal of transcendent dignity is to develop a perfect human being with spiritual health [12]. According to Cheraghi et al, preserving dignity requires respect for the human dignity of patients, which is rooted in their nature as human beings. As a human being, a patient is the Caliph of God (God’s successor in the world) who deserves to be treated with dignity and respect [32]. Bagheri et al define patient dignity as respecting the patient as a unique and valuable human, respecting the equality of all human beings, and displaying respectful behaviour and generosity [40]. Cheraghi et al [41] state that “enlightened practice” is one of the hidden meanings of preserving the dignity of patients. In this regard, providing dignified care offers an opportunity of self-reflection for the nurses to think about the values underlying their practice. Such enlightenment, which is manifested through dignified care, will subsequently lead to a deeper understanding of the value of humanity and promote personal growth in this regard. According to Shahriari et al [42], maintaining the dignity of patients and believing in human dignity means having a humanistic attitude to nursing, to provide ethical care and seeing patients as human beings.
Determining the defining attributesWalker and Avant [35] define attributes as the characteristics that are mentioned frequently when discussing a concept and which help distinguish the concept from other similar or related concepts. According to the literature review, the attributes of dignity include respecting patient’s privacy [29, 33, 39, 42, 43]; observing patient’s solitude; respectful nurse–patient interactions; giving the patient the opportunity to make decisions and participate in decision-making [43, 44]; respecting patients’ autonomy [19, 29, 43, 45]; respecting confidentiality of patient information and observing the principles of respectful communication [19, 43]; reassuring the patient about disease and treatment processes and helping them cultivate a positive mental image [45]; observing the patient’s spiritual or religious beliefs [27, 32]; absence of mental and physical distress symptoms in patients and having peace of mind, independence, and social support [46]; observing patients’ rights, using curtains around the bed during care procedures, and requesting permission before entering the patient’s room [27]; believing in the inherent dignity of human beings, having compassion for the patient [42]. Fundamental dignity includes providing physical and mental safety when providing care; meeting the physical, psychological, and social needs of the patient with the participation of the patient and his/her family members; educating and providing sufficient information to the patient, patient’s family, and other involved people; and having a sense of altruism and maintaining secrecy. Transcendent dignity includes mutual trust between patients, physicians, and nurses; gratitude to God for his blessings and appreciation for the kindness of hospital staff, relatives, and family members; patients’ satisfaction with the provided services; feeling God’s presence [12]; respecting human rationality; having a benevolent attitude; respecting the patient’s personal preferences [32]; using sensitive body language; behaving compassionately; allocating enough time and providing adequate human resources with skill and competence [34]. Other dimensions of dignity include treating the patient as a valuable person and not a goal, instilling a sense of acceptance and love towards the patient, having a professional commitment to protect the patient’s rights [41], providing a safe environment and paying attention to secondary caregivers [33]; paying sufficient attention to patients’ self-esteem, adhering to the principle of human equality, not exhibiting paternalistic behaviour, and not using improper language [11].
Constructing a model
Model case
In this stage of concept analysis, the author presents a real model of the concept to show all its determining attributes. A model case can be a real-world example derived from texts or a hypothetical scenario made up by the researcher [35]. The following is a case based on the researcher’s experience as a tutor.
A 46-year-old man was hospitalised at Shohada Educational and Medical Center in Tabriz following a lumbar disc surgery. To change the dressing for the operation site, we entered the patient’s room with a group of nursing students after obtaining permission from the patient. After greeting him, I introduced myself and the students. Then, while examining the patient’s identification bracelet, I stated the purpose of our presence at the patient’s bed. Before changing the dressing, while one of the students was noting the history of the patient’s illness, the treatment process, and his needs, the patient complained of abdominal pain and nausea since the previous night and that the staff had taken no action despite many follow-ups. After asking the patient for his permission to change the dressing and request his cooperation, the process of changing the dressing and how to cooperate were explained to him to avoid pulling the drain from the operation site and displacing the Foley catheter. As the patient did not feel comfortable in the presence of women, female students left the room. When changing the dressing and when the patient felt comfortable talking to the students, he said, “It is very important to me to regain my health before being discharged. When nurses treat patients like this, it feels as if they want us to leave sooner, as if we want to bother them. Whereas we are all human beings and I did not want to become ill! The last time I was hospitalised in the intensive care unit due to a heart attack. While the nurses were very busy, they would answer our call immediately and treat us kindly and very politely. They would ask the patient’s opinion in every case, so that the decision maker was the patient.” He ended his comment by saying that “they were perfect human beings” and thanked us for listening to him.
In such situations, the needs of patients can be met during hospitalisation. When patients realise that nurses are always available for them, they feel comfortable, satisfied with the delivered service, and feel valued and dignified. Therefore, all the attributes of patient dignity were observed in this case.
Constructing additional cases
Related case
Related cases help researchers understand the network of concepts that surround the main concept. They are examples related to the concept but do not have its defining attributes. The concepts in these related cases are similar to the concept under consideration and are related to it in different ways [35].
A 66-year-old man was diagnosed with Acute Coronary Syndrome and hospitalised in the ICU. He said, “The sound of air conditioning system is not good for those who suffer from heart disease. Some patients do not have a problem with it, but some do. It really bothers me, but it seems that nobody cares. It shows that the hospital is not concerned about patients and does not consider their comfort and convenience. The service staff treat us badly and do not clean the room properly. There were tea stains on the floor yesterday, we had to request cleaning services several times before somebody came and cleaned it.”
The presented case does not display any attributes of the concept of patient dignity; however, because the patient believed that the environmental conditions disturbed his peace and that the behaviour of service staff was not appropriate, it may be confused with the concept of human dignity.
Borderline case
The borderline case has some attributes of the concept but not all of them. In fact, it is an example similar to the model case; however, it lacks some attributes related to the concept [35]. A 16-year-old girl diagnosed with irritable bowel syndrome and hospitalised in the medical ward said: “I was not comfortable because visitors of my roommate enter the room without permission, so that I could not show my blistered legs. We cannot sleep because children cry a lot at night. In the morning, the nurses wake us up for blood tests or doctors want to visit us. That means we can’t control our sleep in the hospital. It is said teenagers can be more intimate with nurses who respect them. I can talk comfortably and intimately with nurses who respect me and my family. I like nurses who call me by my first name.”
This is a borderline model of preserving the human dignity of a patient because some attributes of the concept are covered such as privacy, patient solitude, respect for autonomy, effective communication, and feeling recognised.
Contrary case
According to Walker and Avant [35], the contrary case has no attributes of the main concept, and this difference is quite obvious and is easily recognised by individuals. The following case is the researcher’s observation during his PhD dissertation work and interviews with patients.
The nurse entered the patient’s room and after greeting him, placed the venous catheter replacement equipment on the patient’s bed without explaining the reason for his presence in the room. After examining the current injection site while saying, “Do not shake your hand”, he began to remove injection site tapes and inserted the venous catheter. The patient was worried and probably had no experience of this kind. He asked several questions including “Is it broken?”, “Does it need to be replaced?”, “Can I bear the pain of this one?”, “How long should it be there?”, to find out that the nurse’s goal was to replace the previous venous catheter due to phlebitis. In fact, the nurse did not communicate properly with the patient.
In the above case, none of the attributes of preserving the human dignity of the patient during care are exhibited. It is clear that the present model is contrary to an actual model of preserving human dignity in patients.
Identifying antecedents and consequences
Antecedents
According to Walker and Avant [35], antecedents are events or factors that come before the occurrence of the concept. A review of the literature shows that the concept of human dignity is understood differently by nurses and patients [10, 39, 44]. In this regard, nursing researchers have mentioned various cases of preserving patients’ human dignity during care. The common prerequisites for maintaining human dignity in terms of demographic characteristics of patients include female gender [10, 19, 45], being elder [10,43, 44], being married [10, 27, 44], being employed, having higher education [10, 44], living in a city [27], frequent hospitalisation, patients’ lifestyles (living alone) [10, 45], and nurses’ work experience, which makes them better understand the importance of dignity. Other factors that influence maintaining the dignity of patients are environmental conditions such as safety of patients’ environment; recognising the importance of providing dignified care in that environment [39]; private hospitals [19, 43]; type of medical and intensive care units [10]; the number of patients in the room [43]; and maintenance of the physical space including the availability of basic facilities, cleanliness, lighting of the physical environment [40], hygiene, and noise [33].
Other requirements for respecting the human dignity of patients are paying attention to traditions and culture, the preferences of patients, and religious and personal values [32]. The effects of the religious beliefs of healthcare personnel, increase of smiling during interactions with patients, understanding patients’ feelings, respecting ethical and professional codes of nursing, staff’s skills and competencies [34], intrinsic characteristics, personal beliefs, and quality of the health system structure [40].
Consequences
Consequences are events that result from the occurrence of a concept [35]. Researchers have stated that maintaining the human dignity of patients affects disease outcomes, recovery, and return to normal life [47], and creates a trusting relationship between the nurse and patient [42]. Other studies have reported the consequences of maintaining patients’ human dignity as complete satisfaction with care, feeling closer to God (spiritual growth) [12], maintaining patients’ comfort and trust, [34], and patient satisfaction with the provision of services [40]. Failure to treat patients with dignity makes patients feel indebted, stressed, and embarrassed, which affects their self-esteem [11]. Additionally, other negative consequences of a lack of respect for patients’ human dignity are uncertainty about the disease and treatment process, feelings of being a burden on others, physical distress, anxiety, feeling emotionally incapable of coping with the challenges of the disease, feeling one’s appearance has changed, and inability to perform daily tasks [45].
The antecedents and attributes, as well as the consequences of the concept of human dignity, are summarised in Figure 1.
Figure 1. Conceptual model of human dignity of patients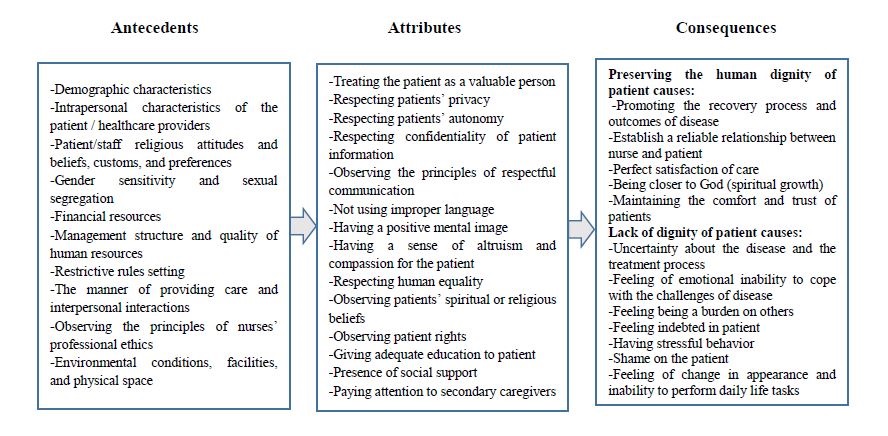
Defining empirical referents is the last stage of concept analysis. Walker and Avant [35] state that empirical referents are classes and categories of actual phenomena and are signs of the occurrence of the concept. In this regard, many qualitative studies have shown different classes of patients’ human dignity. Borhani et al [12], in a qualitative study, showed that the human dignity of patients can be categorised into “fundamental dignity” and “transcendent dignity”. Other categories related to patient dignity are respect for human nature and provision of person-centred care [32], personality, as in personal beliefs and characteristics, communicating behaviours, staff performance related to professional commitment, adequate human resources, skilled and competent staff [34], lack of facilities and equipment, undesirable environmental conditions, cultural and social gaps [33], presence means guaranteeing sufficient attention to patients’ self-esteem [11], observing patient rights, meeting the patient’s spiritual and religious needs, and protecting the privacy of the patient, family and patient-related individuals [42]. Patients believe that all people are equal and that economic status and position do not ensure dignity. Assuring patients that they are valued, by providing respectful service, promotes dignity [40].
Numerous empirical referents on aspects of patients’ human dignity have been reported in the literature. In the tool designed by Karimi [10], a dignity scale is considered to assess the three dimensions of privacy, communication, and autonomy of elder adults and nurses of the elderly. The tool designed by Dehghan-Nayeri et al [44] examines terms related to patients’ dignity in three areas: nurse–adolescent interaction, adolescent privacy, and providing the opportunity for adolescents to make decisions. The translated Patient Dignity Inventory (PDI) by Chochinov et al [47] examines five factors: symptom distress, peace of mind, dependency, social support, and existential distress. The instrument developed by Raee et al [43] to assess the dimensions of privacy and independence of the patient’s dignity is in accordance with the sociocultural conditions of Iranian society [45, 46]. Other designed tools are — the questionnaire designed by Zirak et al, based on a literature review and in accordance with the ethical laws of Iranian nursing to assess patients’ dignity [27], and a researcher-made tool, that covers important aspects of care affecting human dignity in an aged population [39].
The authors conclude that the attributes of the concept of human dignity are abstract, and they have found no independent tool to measure all the aspects of this concept. Therefore, to create a comprehensive definition of human dignity of patients in nursing care, it is necessary to conduct further studies to develop other empirical referents based on this analysis.
Discussion
The Walker and Avant model provides a systematic approach to identify and clarify the concept of human dignity of patients in nursing care. It also helps researchers identify specific and distinctive attributes of the concept and develop a deeper understanding of its meaning by constructing a model case, borderline case, related case, and contrary case.
The concept of dignity is constituted by two distinct sets of human characteristics — human security, comprehensive care, giving adequate information to the patients and their families, and respecting the patient as a human being, along with altruism, effective communication, and maintenance of privacy. These ensure the physical and mental health of the patient and fall under the category of fundamental dignity. Characteristics such as trust, gratitude, and spiritual growth fall under the category of transcendent dignity. The goal of transcendent dignity is to develop a perfect human with spiritual health. The subjective human dignity of patients is rooted in their nature as human beings and the caliph of God (God’s successors in the world), who deserve to be treated with dignity and respect. The different dimensions of patient dignity are respecting human rationality, exercising equality, having a benevolent attitude, and spending time with the patient. Provision of objective and person-oriented dignified care includes respect for cultural and religious values and consideration of personal preferences, with the latter being influenced by cultural and religious values and beliefs. Asmaningrum and Tsai described four main categories of nursing care to maintain patient dignity in a clinical care setting: responsiveness, maintaining a respectful nurse–patient relationship, quality of care, and providing individualised care [25]. They also stated that it is important for nurses to have clinical skills along with relevant cultural competencies. According to the International Code of Ethics for Nurses, respecting life and observing dignity are integral to the nursing profession, and this is not limited by the age, colour, belief, culture, gender, nationality, race, social status, or health status of the patient [14].
Other important dimensions and attributes of patient dignity identified in this study were the observance of patient privacy, respect for autonomy, respectful nurse–patient interactions, patient participation in decision-making, absence of mental and physical distress symptoms in patients, having peace of mind, independence, social support, acceptance and observance of patient rights, requesting permission before entering the patient’s room by staff, compassion for the patient, benignity and altruism, professional commitment to protect patients’ rights and enlightened practice, providing a safe environment, attention to secondary caregivers and sufficient attention to patients’ self-esteem. The results of Šaňáková and Čáp showed six main themes related to patients’ dignity regarding elderly adults: unique human beings, respect for patient privacy and solitude, quality of relationships, quality of communication, quality of care, and environment [48]. Lin and Tsai identified five themes: respect, privacy, emotional support, equal treatment of all patients, and maintaining body image [49]. In this study, the aspects of respect were autonomy, comprehensive care, culture and beliefs, and informed consent. The aspects of privacy include the privacy of the patient’s body, physical space, and conditions. The aspects of emotional support are using encouraging words, listening to patients and exercising empathy, not using improper language, and cultivating spiritual well-being. The aspects of equal treatment of all patients are providing equal care. The aspect of maintaining body image is physical appearance.
Solberg and Nåden reported three main themes of dignity: the physical dimension, respect for others, and internal experience [50]. According to this study, respect and approval, providing care with knowledge, and maintaining a continuous relationship with the patient were among the factors that increase patient dignity. Discrimination, inappropriate communication, patient disapproval, disrespect, a negative attitude, lack of support, and lack of knowledge were reported as factors threatening patient dignity.
In summary, upholding dignity is the fundamental mission of the nursing profession. Dignity is the intrinsic value of human beings, inviolably and inextricably tied to their full, vivid existence. Dignity is owed regard and respect, whether it is respect for vulnerability, admiration for superiority, or relational confirmation in everyday reality [51].
Based on the results of the present study, demographic characteristics, environmental conditions, patients’ religious preferences and beliefs, nurses’ behaviour, and hospital rules were found to be most important factors influencing the maintenance and promotion of patients’ dignity while providing care. According to the findings of Martin-Ferreres et al, nurses’ attitudes and behaviours are important for providing dignified care with respect, confidentiality, privacy, and communication [24]. Institutional policies and management of emotions were also identified as facilitators and threatening factors in providing dignified care. According to Rasmussen and Delmar, the factors affecting patients’ dignity are respect for privacy, autonomy, meeting the patient needs, opportunity to choose, openness, loyalty and confidence in interactions, providing sufficient information, use of resources, dependence to others and losing control, and behaviour and communication skills in nurses [52]. In other review study conducted by Lin et al the findings showed that from the perspective of nurses and patients, maintaining patients’ dignity in providing care in clinical settings is influenced by physical space of the environment, staff attitude and behaviour, organisational culture, and patient independency [6].
Hence, dignity has many dimensions and attributes that are represented by various factors. Patients have a clear understanding of the factors affecting dignity. At the same time, they expect healthcare providers to maintain dignity while providing care. Additionally, nurses must recognise the various aspects of preserving the value and importance of patients, as well as the ethical dimension of their activities in clinical practice that contribute to the esteem and dignity of patients.
Limitations
Only texts published in English or Persian were included. Accordingly, texts in other languages, as well as unpublished data on human dignity and those published prior to 2010 were not analysed. However, analysing this concept is an ever-changing process, and the newly discovered aspects need further research work.
Conclusion
According to the findings of the present study, the meaning of patients’ dignity was determined in two dimensions. One dimension is intrinsic or fundamental dignity that exists for all human beings and is objective. The second dimension is the acquired dimension or transcendent dignity that is subjective and has as its goal the development of a human being in perfect spiritual health. The antecedents of patients’ human dignity provide general evidence of several factors. Considering the fact that dignity is evident through special attributes, nurses, by recognising the concept of dignity and its features, can include various aspects of dignity in their daily care activities. Regarding the consequences of patients’ human dignity, this study developed a base for an operational definition of the concept of human dignity that nurses need to take it into account while providing care. Understanding the relationship between the antecedents, attributes, and consequences of patients’ human dignity can help in designing a framework for education in the field of ethical competencies in nursing. The subject of human dignity, as included in the nursing curriculum, is limited, and a practical credit for practising dignified care at the patient’s bedside can help prepare future nurses to promote a culture of dignified and ethical care.
The findings of this study can be used in international and national discussions on nursing and future studies on interventions to promote a culture of ethical and dignified care. It is also suggested that future research should cover how the views of nursing professors act as a model for students in understanding the human dignity of patients.
Conflict of interest and funding: None declared.
References
- Hughes G. The concept of dignity in the universal declaration of human rights. J Relig Ethics. 2011 Mar;39(1):1-24. https://doi.org/10.1111/j.1467-9795.2010.00463.x
- United Nations General Assembly. Universal declaration of human rights. Paris: UNGA. 1948 Dec 10 [cited Feb 2020]. Available from: https://www.un.org/en/about-us/universal-declaration-of-human-rights
- Esmaieli R, Abed Saeedi J, Ashktorab T, Esmaili M. Concept of elderly dignity in nursing perspective: a systematic review. Med Hist.2014[cited Feb 2020];5(17):11-36. Available from: https://www.sid.ir/en/journal/ViewPaper.aspx?id=353516
- Johnston B, Pringle J, Gaffney M, Narayanasamy M, McGuire M, Buchanan D. The dignified approach to care: a pilot study using the patient dignity question as an intervention to enhance dignity and person-centred care for people with palliative care needs in the acute hospital setting. BMC Palliat Care. 2015 Apr 9;14(1):1-14. https://doi.org/10.1186/s12904-015-0013-3 Heijkenskjöld KB, Ekstedt M, Lindwall L. The patient’s dignity from the nurse’s perspective. Nurs Ethics. 2010 May;17(3):313-24. https://doi.org/10.1177/0969733010361444
- Lin Y-P, Watson R, Tsai Y-F. Dignity in care in the clinical setting: a narrative review. Nurs Ethics. 2013 Mar;20(2):168-77. https://doi.org/10.1177/0969733012458609
- Jacobson N. Dignity violation in health care. Qual Health Res. 2009 Nov;19(11):1536-47. https://doi.org/10.1177/1049732309349809
- Gastmans C. Dignity-enhancing nursing care: a foundational ethical framework. Nurs Ethics. 2013 Mar;20(2):142-9. https://doi.org/10.1177/0969733012473772
- Lindwall L, von Post I. Preserved and violated dignity in surgical practice–nurses’ experiences. Nurs Ethics. 2014 May;21(3):335-46. https://doi.org/10.1177/0969733013498527
- Karimi H, Ajorpaz NM, Aghajani M. Older adults’ and nurses’ perception of dignity in the setting of Iranian hospitals: a cross-sectional study. Cent Eur J Nurs Midw. 2019 Sep;10(4):1134-42. https://doi.org/10.15452/CEJNM.2019.10.0025
- Bidabadi FS, Yazdannik A, Zargham-Boroujeni A. Patient’s dignity in intensive care unit: a critical ethnography. Nurs Ethics. 2019 May;26(3):738-52. https://doi.org/10.1177/0969733017720826
- Borhani F, Abbaszadeh A, Rabori RM. New vision for the dignity: understanding the meaning of patient dignity in Iran. Br J Med Med Res. 2015 Jun;9(2):1-11. https://doi.org/10.9734/BJMMR/2015/18886
- Bell L. Code of ethics for nurses with interpretive statements. Crit Care Nurse. 2015 Aug;35(4):84. https://doi.org/10.4037/ccn2015639
- International Council of Nurses. The International Code of Ethics for Nurses. 2012; Geneva: International Council of Nurses. 4th ed.
- Jolaee S, Bakhshandeh B, Mohammadebrahim M, Asgarzadeh, M, Vasheghanifarahani, A, Shariat, E. Nursing code of ethics in Iran: the report of an action research. J Med Ethics Hist Med. 2010[cited Feb 2020];3(2):45-53. Available from: https://ijme.tums.ac.ir/article-1-5024-en.html
- Baillie L, Gallagher A. Raising awareness of patient dignity. Nurs Stand. 2012 Oct;27(5):44-49. https://doi.org/10.7748/ns2012.10.27.5.44.c9333
- Royal College of Nursing. Principles of nursing practice: an RCN guide to principles of nursing practice. RCN, London. 2018 [cited 30 July 2018]. Available from: https://www.rcn.org.uk/Professional-Development/Principles-of-nursing-practice
- Jackson A, Irwin W. Dignity, humanity and equality: principle of nursing practice A. Nurs Stand. 2011 Mar;25(28):35-37. https://doi.org/10.7748/ns2011.03.25.28.35.c8396
- Raee Z, Abedi H. Nurses’ perspectives on human dignity of hospitalized patients. Iran J Nurs. 2017;29(104):55-65. https://doi.org/10.29252/ijn.29.104.55
- Tranvåg O, Synnes O, McSherry W. Stories of dignity within healthcare: research, narratives and theories. Cumbria: M&K Update Ltd; 2016.
- Sabatino L, Kangasniemi MK, Rocco G, Alvaro R, Stievano A. Nurses’ perceptions of professional dignity in hospital settings. Nurs Ethics. 2016 May;23(3):277-93. https://doi.org/10.1177/0969733014564103
- Thompson GN, McArthur J, Doupe M. Identifying markers of dignity-conserving care in long-term care: a modified Delphi study. PLoS One. 2016 Jun;11(6):e0156816. https://doi.org/10.1371/journal.pone.0156816
- Rodríguez-Prat A, Monforte-Royo C, Porta-Sales J, Escribano X, Balaguer A. Patient perspectives of dignity, autonomy and control at the end of life: systematic review and meta-ethnography. PLoS One. 2016 Mar;11(3):e0151435. https://doi.org/10.1371/journal.pone.0151435
- Martin-Ferreres ML, Pardo MÁDJ, Porras DB, Moya JLM. An ethnographic study of human dignity in nursing practice. Nurs Outlook. 2019 Jul-Aug;67(4):393-403. https://doi.org/10.1016/j.outlook.2019.02.010
- Asmaningrum N, Tsai YF. Patient perspectives of maintaining dignity in Indonesian clinical care settings: a qualitative descriptive study. J Adv Nurs. 2018 Mar;74(3):591-602. https://doi.org/10.1111/jan.13469
- Parandeh A, Khaghanizade M, Mohammadi E, Mokhtari-Nouri J. Nurses’ human dignity in education and practice: an integrated literature review. Iran J Nurs Midwifery Res. 2016 Jan-Feb;21(1):1-8. https://doi.org/10.4103/1735-9066.174750
- Zirak M, Ghafourifard M, Aliafsari Mamaghani E. Patients’ dignity and its relationship with contextual variables: a cross-sectional study. J Caring Sci. 2017 Mar;6(1):49-51. https://doi.org/10.15171/jcs.2017.006
- Bagherian S, Sharif F, Zarshenas L, Torabizadeh C, Abbaszadeh A, Izadpanahi P. Cancer patients’ perspectives on dignity in care. Nurs Ethics. 2020 Feb;27(1):127-40. https://doi.org/10.1177/0969733019845126
- Jamalimoghadam N, Yektatalab S, Momennasab M, Ebadi A, Zare N. Hospitalized adolescents’ perception of dignity: a qualitative study. Nurs Ethics. 2019 May;26(3):728-37. https://doi.org/10.1177/0969733017720828
- Tehranineshat B, Rakhshan M, Torabizadeh C, Fararouei M. Patient dignity in Iranian clinical care settings as perceived by physicians, caregivers, and patients. J Multidiscip Healthc. 2020 Sep;13:923-933. https://doi.org/10.2147/JMDH.S258962
- Parandeh A. The necessity of preserving human dignity of patients in intensive care units: letter to the editor. J Crit Care Nurs. 2019[cited Feb 2020];12(3):1-5. Available from: http://jccnursing.com/article-1-462-en.html
- Cheraghi MA, Manookian A, Nasrabadi AN. Human dignity in religion-embedded cross-cultural nursing. Nurs Ethics. 2014 Dec;21(8):916-28. https://doi.org/10.1177/0969733014521095
- Ebrahimi H, Torabizadeh C, Mohammadi E, Valizadeh S. Patients’ perception of dignity in Iranian healthcare settings: a qualitative content analysis. J Med Ethics. 2012;38(12):723-8. http://dx.doi.org/10.1136/medethics-2011-100396
- Manookian A, Cheraghi MA, Nasrabadi AN. Factors influencing patients’ dignity: a qualitative study. Nurs Ethics. 2014 May;21(3):323-34. https://doi.org/10.1177/0969733013498526
- Walker LO, Avant KC. Strategies for theory construction in nursing. 5th Ed. Upper Saddle River, NJ: Prentice Hall; 2011
- Misztal BA. The idea of dignity: its modern significance. Eur J Soc Theory. 2013 Feb;16(1):101-21. https://doi.org/10.1177/1368431012449237
- Afzali MA. Human dignity and euthanasia in Islamic ethics. J Mazandaran Univ Med Sci. 2010 May[cited Feb 2020];20(78):83-95. Available from: http://jmums.mazums.ac.ir/article-1-629-en.html
- Esmaili R, Ashktorab T, Esmaili M, Rais Yazdi H, Jamalodini S. Philosophy of human relationships and ethics in medical sciences. Med Ethics. 2011[cited Feb 2020];5(16):79-93. Available from: https://www.sid.ir/en/Journal/ViewPaper.aspx?ID=208388
- Sabeghi H, Nasiri A, Zarei M, Tabar A K, Golbaf D. Respecting for human dignity in elders caring in perspective of nurses and elderly patients. Med Ethics. 2017[cited Feb 2020];9(32):45-70. Available from: https://www.magiran.com/paper/1438696?lang=en
- Bagheri H, Yaghmaei F, Ashktorab T, Zayeri F. Patient dignity and its related factors in heart failure patients. Nurs Ethics. 2012 May;19(3):316-27. https://doi.org/10.1177/0969733011425970
- Cheraghi MA, Manookian A, Nasrabadi AN. Patients’ lived experiences regarding maintaining dignity. J Med Ethics Hist Med. 2015[cited Feb 2020];8:6. Available from: https://philpapers.org/rec/CHEPLE-2
- Shahriari M, Mohammadi E, Abbaszadeh A, Bahrami M, Fooladi M M. Perceived ethical values by Iranian nurses. Nurs Ethics. 2012 Jan;19(1):30-44. https://doi.org/10.1177/0969733011408169
- Raee Z, Abedi H, Shahriari M. Nurses’ commitment to respecting patient dignity. J Educ Health Promot. 2017;6:16. https://doi.org/10.4103/2277-9531.204743
- Dehghan Nayeri N, Karimi R, Sadeghee T. Iranian nurses and hospitalized teenagers’ views of dignity. Nurs Ethics. 2011 Jul;18(4):474-84. https://doi.org/10.1177/0969733011403552
- Borhani F, Abbaszadeh A, Rabori RM. Facilitators and threats to the patient dignity in hospitalized patients with heart diseases: a qualitative study. Int J Community Based Nurs Midwifery. 2016 Jan[cited Feb 2020];4(1):36-46. Available from: https://ijcbnm.sums.ac.ir/article_40727.html
- Amininasab SS, Lolaty HA, Moosazadeh M, Shafipour V. The relationship between human dignity and medication adherence in patients with heart failure. J Med Ethics Hist Med. 2017[cited Feb 2020];10:5. Available from: https://jmehm.tums.ac.ir/index.php/jmehm/article/view/248
- Borhani F, Abbaszadeh A, Moosavi S. Status of human dignity of adult patients admitted to hospitals of Tehran. J Med Ethics Hist Med. 2014[cited Feb 2020];7:20. Available from: https://jmehm.tums.ac.ir/index.php/jmehm/article/view/122
- Šaňáková Š, Čáp J. Dignity of elderly adults from the perspective of nurses: a qualitative descriptive study. Cent Eur J Nurs Midw. 2018[cited Feb 2020];9(4):906-14. https://doi.org/10.15452/CEJNM.2018.09.0023
- Lin YP, Tsai YF. Maintaining patients’ dignity during clinical care: a qualitative interview study. J Adv Nur. 2011 Feb; 67(2): 340-8. https://doi.org/10.1111/j.1365-2648.2010.05498.x
- Solberg H, Nåden D. It is just that people treat you like a human being: The meaning of dignity for patients with substance use disorders. J Clin Nurs. 2020 Feb;29(3-4):480-91. https://doi.org/10.1111/jocn.15108
- Cho AN. Beholding & upholding human dignity in the nursing profession. Veritas: Villanova Research Journal. 2020 Sep[cited Feb 2020];2:28-42. Available from: https://jche.journals.villanova.edu/index.php/veritas/article/view/2457
- Rasmussen TS, Delmar C. Dignity as an empirical lifeworld construction—in the field of surgery in Denmark. Int J Qual Stud Health Well-being. 2014;9(1):24849. https://doi.org/10.3402/qhw.v9.24849