RESEARCH ARTICLE
Global disparities and data transparency in editorial boards of prominent Internal medicine journals including allied super specialities: A wake-up call
Jasmeet Singh, Pratyush Kumar, Abhishek Kumar
Published online first on June 3, 2025. DOI:10.20529/IJME.2025.045Abstract
Background: Global healthcare research suffers from inequalities, favouring high-income countries, which hampers fair healthcare access. Low and lower-middle-income nations face limited participation and editorial bias, posing concerns for research integrity. Potential reasons for this pattern might be the overrepresentation of researchers from the Global North on editorial boards, disparities in the quality of scientific research, lack of support for local research initiatives, and challenges posed by language barriers. The aim of this study was to assess data transparency and representation patterns of low- and lower-middle-income nations on Editorial Boards of prominent Internal Medicine journals.
Methods: The top 50 journals in the “Internal medicine including allied super specialities” subject category were selected based on SCImago journal ranking, journal impact factor, literature research and journal citation report. We examined the editorial boards of these journals using the World Bank Income Criteria.
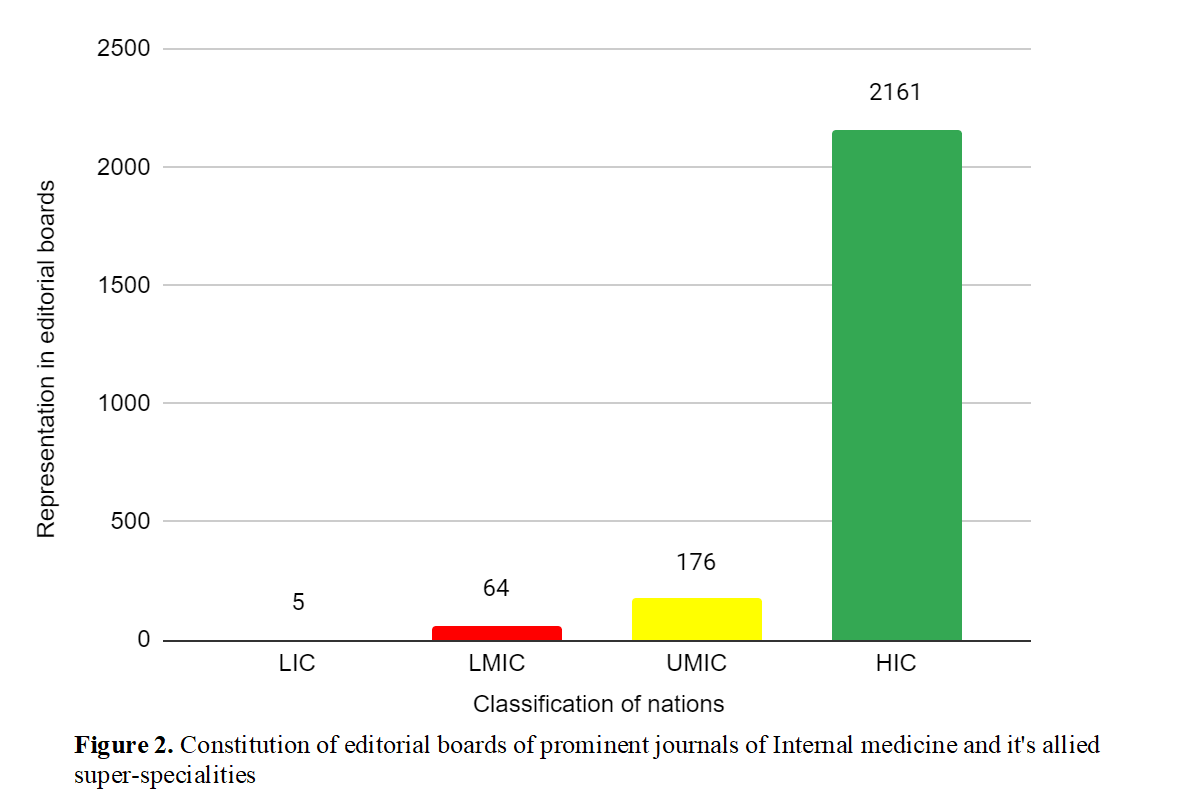
Results: Out of 2406 editorial board members of leading journals, only 5(0.21%) were from low-income countries (LICs), while lower-middle-income countries (LMICs) and upper-middle- income countries (UMICs) constituted 64(2.67%) and 176(7.31%), respectively. High-income countries (HICs) dominated editorial boards, with 2161(89.8%) representation.
Conclusion: Editorial boards of top Internal Medicine and allied super-specialty journals lack adequate representation from low and lower-middle-income countries. This deficiency has significant implications, affecting knowledge production, policy development, and the overall progress of science and research on a global scale. Urgent measures are required to establish a fair and inclusive scholarly publishing system that caters to researchers from all regions.
Keywords: global disparity, editorial board, LICs, research ethics, internal medicine, global north
Introduction
Countries are categorised by income into high-income countries (HICs), upper-middle-income countries (UMICs), lower-middle-income countries (LMICs) and low-income countries (LICs), according to the World Bank’s income criteria [1]. Global disparities in healthcare research have been a longstanding concern, as HICs frequently dominate the field, often overshadowing the contributions from LICs and LMICs. This power imbalance not only perpetuates inequalities but also hinders the development of effective healthcare solutions tailored to the unique needs of less privileged regions. LICs and LMICs encounter a number of obstacles as they strive to make substantial contributions to worldwide healthcare research endeavours.
In recent years, the scientific contribution from LICs and LMICs to indexed publications has remained limited. A study by Aluede et al [2] found that out of 3,964 publications analysed, only 7% included authors from LICs and LMICs, with the vast majority coming from industrialised and emerging-market economies. Notably, while Sub-Saharan Africa contributed only 0.4% of all articles overall, it accounted for 5.6% of the 265 articles that included authors from LICs and LMICs, underscoring the limited collaboration occurring specifically within LICs and LMICs. In a cross-sectional, survey-based study, Rohra [3] surveyed corresponding authors of pharmacology papers and reported that 584 (30.4% of the 1,919 papers) originated from Least Developed Countries (LDCs), with a 64.5% author response rate. Approximately half of LDC papers were in low-impact factor journals, showing a weak negative correlation (r = -0.236) between journal impact factor and LDC representation. Another study by Saxena et al [4] showed similar results. This imbalance in representation has led to a situation reminiscent of global North colonisation, where researchers from HICs dominate major decision-making processes, often leaving their counterparts from LICs and LMICs without the platform they rightfully deserve. This issue raises important concerns, as it inadvertently excludes a substantial portion of the global population residing in these nations. Notably, five of the world’s ten most populous countries, including India, Indonesia, Pakistan, Nigeria, and Bangladesh, fall into the category of LICs and LMICs, as noted by Hamadeh et al [5]. This disparity in research representation raises critical questions about equity and access to healthcare advancement for a significant proportion of the world’s population. Addressing this imbalance is not only a matter of global health ethics but also crucial for achieving comprehensive healthcare solutions worldwide.
In diseases endemic to LICs and LMICs, a prevalent pattern emerges: the literature is predominantly reviewed by editorial boards composed of physicians from UMICs and HICs. While the causes of this contrast vary worldwide, a common thread is the presence of editorial bias and a deficiency in scientific enthusiasm, as discussed by Rohra [3]. Importantly, this disparity across the editorial boards of different journals can potentially result in erroneous conclusions and numerous biases, emphasising the need for a more equitable representation of perspectives and expertise in the field.
This emerging pattern also amplifies concerns about whether authors from more privileged economies are using these regions as testing grounds for their research, due to the diverse patient populations available. While a significant portion of infectious disease research occurs in LICs and LMICs due to the prevalence of such diseases, a study analysing authorship trends in infectious diseases articles published from 1998 to 2018 noted a concerning increase in the exclusion of first authors with low-income background affiliations [6]. It is important to mention that local physicians from these regions, who would possess valuable insights into the conditions discussed, have reported perceiving editorial bias against them solely because of their geographical location [7]. This skewed representation also carries serious implications.
Additionally, research indicates that the epidemiologically prevalent diseases in these regions are often inadequately described in published articles [8]. As a result, the local risk factors that significantly affect the management and prognosis of these diseases remain poorly understood. This highlights a substantial gap between the expertise available and the practical requirements faced by physicians working in these non HICs.
The underrepresentation of LICs and LMICs goes beyond article publication and impacts corresponding authorship, journal indexations, and citations, as illustrated by Rohra [3]. The research revealed that 76.5% of authors face challenges in publishing in quality journals within their countries due to editor and reviewer bias (64.8%) and the poor English writing skills of scientists of LICs and LMICs (52.8%). A bibliometric analysis by Igoumenou et al [9], focusing on the field of psychiatry, examined geographic trends in scientific output and citation practices. The study found that the majority of publications originated from the USA, followed by Germany and the UK in terms of productivity. Articles from the USA also received the highest number of citations, averaging 11.5 citations per article. While the UK had the second-highest total number of citations, it ranked fourth in citation rate (9.7 citations per article), with the Netherlands (11.4 citations per article) and Canada (9.8 citations per article) leading in this metric. Another study by Mari et al [10] highlighted similar problems. These studies [2,3, 6, 9, 10] consistently reveal a notable trend: a significant majority of editorial board members in top journals are predominantly from the Global North. Editorial boards significantly influence academic publishing, and the underrepresentation of scholars from LICs and LMICs is a pressing concern. While our study focuses on internal medicine journals, it is important to acknowledge that these challenges are pervasive across various disciplines. Although research has examined editorial board composition in specific clinical specialties [11, 12] , there remains a notable gap in the literature regarding internal medicine. Internal medicine journals hold a unique position due to the field’s broad and foundational nature, covering a wide range of diseases affecting diverse global populations. Equitable representation on these editorial boards is crucial to ensure that research priorities reflect global health needs, particularly those prevalent in LMICs. The absence of such representation risks narrowing the scope of published research and overlooking significant health challenges in these regions. By focusing on internal medicine, this study aims to address the specific dynamics of underrepresentation within the field, particularly on how these issues intersect with peer review processes. This targeted investigation not only sheds light on studies in internal medicine but also offers insights that could apply to other disciplines facing similar challenges. Ultimately, our findings seek to promote a more inclusive and equitable academic publishing environment across all fields, by bridging the existing gap in internal medicine journals.
Methods
Study designIt is a descriptive study regarding editorial board composition of leading international journals in medicine.
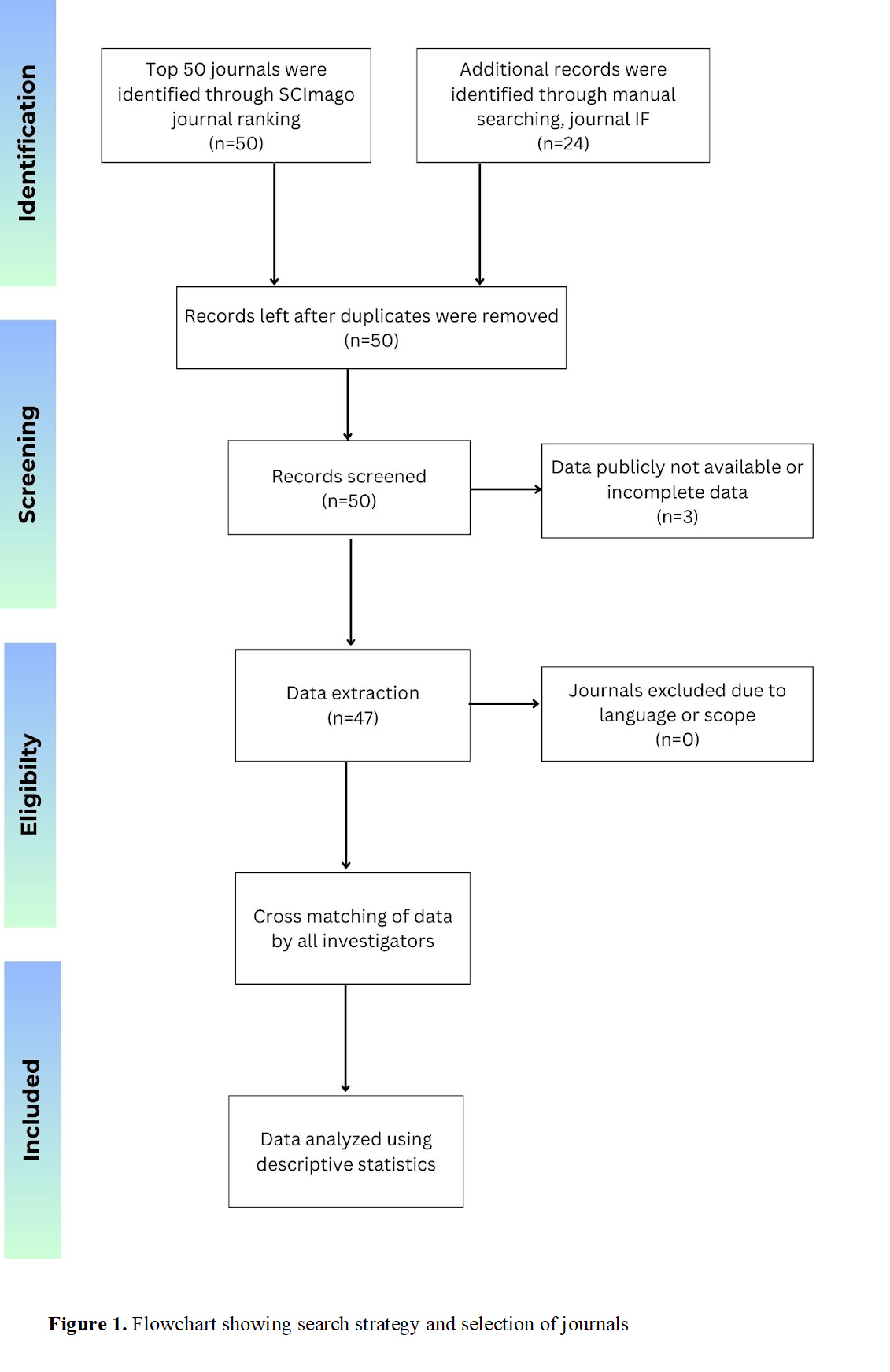
Search strategyWe identified the top 50 journals in the “Internal medicine including allied super specialities” subject category, as determined by their SCImago journal ranking. Through manual internet searching, we also identified the list of journals by impact factor and also the journal citation report. All the journals were imported into an excel sheet and duplicates removed to identify the top 50 journals overall with consensus.
Inclusion and exclusion criteriaThe study included journals primarily focused on “Internal medicine including allied super specialities”. We specifically selected international journals, which published studies from different regions, rather than solely focusing on regional or national publications. This allowed us to explore the representation of diverse nations. Journals that identified themselves on generic healthcare sciences were excluded. This was done by thematic analysis of the “scope” section of the journal and independent voting by each author. In case of any disagreement, the journal was emailed to get their opinion considering the targeted scope of the paper. Journals that are not published primarily in the English language were also excluded from the study. In the process of data extraction, if the journal website lacked information about its board composition or failed to report the respective countries of its editorial board members, this was documented. We strictly utilised only the journal website and journals’ responses to our emails, while excluded other third-party websites giving information about the editorial board. Moreover, if attempts to extract this data via email outreach were unsuccessful, this was also noted in the study results as part of the transparency assessment.
Data extractionThe official website of the journal was manually searched separately by two investigators who plotted the composition of the Editorial Board into excel sheets. The sheets were matched and upon disagreement in numbers, the third investigators rechecked the composition of the journal editorial board. The list was arranged as per SCImago Journal Ranking to avoid any bias. It is worth noting that the SCImago journal ranking considers the open-access nature of manuscripts and relies on a comprehensive source database, along with an evaluation of citation quality, as its distinctive features. This has been validated scientifically by Falagas et al [13]. We screened these journals according to specific inclusion and exclusion criteria. Search strategy and Selection of journals is summarised in Figure 1 (available online only).
Results
Based on our search strategy, 50 journals were identified in ranking. Data was extracted from 47 journals, as the remaining three journals either lacked information about their editorial board composition or had incomplete data on their publicly accessible websites. A total of 2406 editorial board members were identified from the selected journals included in our study. A miniscule contribution of 0.21% (5) editorial board members were from LICs, while percent composition for LMICs and UMICs were 2.67% (64) and 7.31% (176), respectively. HICs had a huge participation of 89.8% (2161) of board members. Extracted data is tabulated and represented in Table 1 and Figure 2 (available online only), respectively. Only 3(6.4%) journals had a member from LIC. Sixty percent of LIC members were from a single journal (Cardiovascular Diabetology) and the remaining 40% LIC members were from the remaining two journals. Twenty-one journals had a minimum of one member from LMIC. Gender information for editorial board members was not consistently available on the publicly accessible websites of the selected journals. As a result, gender analysis could not be included in the study.
Table 1. Composition of editorial boards of top 50 Internal medicine journals
|
S. No. |
Journal |
SJR |
H index |
Total Number of Editorial Board Members |
LIC |
LMIC |
UMIC |
HIC |
|
1 |
The Lancet Diabetes and Endocrinology |
9.767 Q1 |
132 |
3 |
0 |
0 |
0 |
3 |
|
2 |
Diabetes Care |
6.528 Q1 |
380 |
36 |
0 |
0 |
0 |
36 |
|
3 |
Nature Metabolism |
6.201 Q1 |
41 |
5 |
0 |
0 |
0 |
5 |
|
4 |
JAMA Internal Medicine |
5.772 Q1 |
358 |
18 |
0 |
0 |
0 |
18 |
|
5 |
Annals of Internal Medicine |
4.621 Q1 |
403 |
28 |
0 |
0 |
0 |
28 |
|
6 |
Diabetologia |
3.528 Q1 |
241 |
22 |
0 |
0 |
0 |
22 |
|
7 |
Hypertension |
3.395 Q1 |
276 |
52 |
0 |
1 |
3 |
48 |
|
8 |
Journal of Internal Medicine |
3.193 Q1 |
170 |
39 |
0 |
0 |
2 |
37 |
|
9 |
JHEP Reports |
2.835 Q1 |
19 |
60 |
0 |
2 |
6 |
52 |
|
10 |
Diabetes |
2.776 Q1 |
345 |
Data publicly available but incomplete (accessed on 18 Nov 2023) |
||||
|
11 |
Cardiovascular Diabetology |
2.449 Q1 |
85 |
66 |
3 |
3 |
8 |
52 |
|
12 |
Diabetes, Obesity and Metabolism |
2.356 Q1 |
135 |
31 |
0 |
0 |
2 |
29 |
|
13 |
The Lancet Regional Health – Western Pacific |
2.008 Q1 |
9 |
4 |
0 |
0 |
2 |
2 |
|
14 |
Paediatric Diabetes |
1.942 Q1 |
82 |
59 |
0 |
1 |
4 |
54 |
|
15 |
Diabetes and Metabolism |
1.834 Q1 |
94 |
29 |
0 |
1 |
1 |
27 |
|
16 |
Diabetes/Metabolism Research and Reviews |
1.781 Q1 |
117 |
85 |
0 |
0 |
9 |
76 |
|
17 |
Amyloid: the international journal of experimental and clinical investigation: the official journal of the International Society of Amyloidosis |
1.706 Q1 |
65 |
60 |
0 |
0 |
0 |
60 |
|
18 |
Diabetes Research and Clinical Practice |
1.677 Q1 |
122 |
56 |
0 |
6 |
7 |
43 |
|
19 |
Diabetes and Metabolic Syndrome: Clinical Research and Reviews |
1.587 Q1 |
56 |
45 |
0 |
20 |
2 |
23 |
|
20 |
Current Diabetes Reports |
1.577 Q1 |
85 |
27 |
0 |
2 |
3 |
22 |
|
21 |
Journal of General Internal Medicine |
1.537 Q1 |
192 |
87 |
0 |
0 |
1 |
86 |
|
22 |
Current Hypertension Reports |
1.413 Q1 |
79 |
55 |
0 |
3 |
10 |
42 |
|
23 |
Diabetic Medicine |
1.405 Q1 |
152 |
43 |
0 |
2 |
4 |
37 |
|
24 |
Journal of Clinical Lipidology |
1.281 Q1 |
62 |
91 |
0 |
0 |
1 |
90 |
|
25 |
IEEE Transactions on Neural Systems and Rehabilitation Engineering |
1.257 Q1 |
148 |
66 |
0 |
2 |
7 |
57 |
|
26 |
Journal of Atherosclerosis and Thrombosis |
1.245 Q1 |
76 |
143 |
0 |
0 |
1 |
142 |
|
27 |
European Journal of Internal Medicine |
1.210 Q1 |
79 |
64 |
0 |
0 |
6 |
58 |
|
28 |
Nutrition and Diabetes |
1.202 Q1 |
45 |
23 |
0 |
1 |
2 |
20 |
|
29 |
Journal of diabetes science and technology |
1.142 Q1 |
81 |
Data not publicly available (accessed on 18 Nov 2023)
|
||||
|
30 |
Hypertension Research |
1.119 Q1 |
95 |
49 |
0 |
0 |
3 |
46 |
|
31 |
Diabetology and Metabolic Syndrome |
1.118 Q1 |
55 |
32 |
0 |
2 |
17 |
13 |
|
32 |
Journal of Hypertension |
1.107 Q1 |
178 |
132 |
1 |
0 |
12 |
119 |
|
33 |
Journal of Diabetes and its Complications |
1.057 Q1 |
88 |
45 |
0 |
1 |
1 |
43 |
|
34 |
Acta Diabetologica |
1.048 Q1 |
73 |
12 |
0 |
0 |
0 |
12 |
|
35 |
Journal of Hospital Medicine |
1.033 Q2 |
71 |
60 |
0 |
0 |
1 |
59 |
|
36 |
Current Opinion in Nephrology and Hypertension |
0.968 Q2 |
97 |
23 |
0 |
2 |
1 |
20 |
|
37 |
Pregnancy Hypertension |
0.950 Q2 |
29 |
26 |
0 |
0 |
1 |
25 |
|
38 |
Journal of Diabetes Investigation |
0.932 Q2 |
55 |
84 |
0 |
0 |
8 |
76 |
|
39 |
OpenNano |
0.932 Q2 |
14 |
26 |
0 |
0 |
6 |
20 |
|
40 |
Diabetes Therapy |
0.902 Q2 |
38 |
28 |
0 |
1 |
1 |
26 |
|
41 |
Clinical Medicine Insights: Endocrinology and Diabetes |
0.879 Q2 |
18 |
Data not publicly available (Accessed on 18 Nov 2023)
|
||||
|
42 |
Kidney Medicine |
0.876 Q2 |
12 |
70 |
0 |
7 |
5 |
58 |
|
43 |
Journal of Clinical Hypertension |
0.875 Q2 |
70 |
78 |
1 |
2 |
19 |
57 |
|
44 |
Canadian Journal of Diabetes |
0.873 Q2 |
42 |
29 |
0 |
0 |
0 |
29 |
|
45 |
American Journal of Hypertension |
0.862 Q2 |
141 |
98 |
0 |
2 |
3 |
93 |
|
46 |
Internal and Emergency Medicine |
0.861 Q2 |
51 |
85 |
0 |
0 |
5 |
80 |
|
47 |
Endocrine Connections |
0.839 Q2 |
29 |
36 |
0 |
0 |
3 |
33 |
|
48 |
Current Opinion in Endocrinology, Diabetes and Obesity |
0.814 Q2 |
72 |
22 |
0 |
0 |
0 |
22 |
|
49 |
Korean Circulation Journal |
0.810 Q2 |
32 |
109 |
0 |
2 |
4 |
103 |
|
50 |
Pancreas |
0.804 Q2 |
109 |
64 |
0 |
1 |
5 |
58 |
|
Total |
|
|
2406 |
5 |
64 |
176 |
2161 |
|
|
Note: SJR: SCImago Journal Ranking indicator, H index: Hirsch index; LIC: Low-income countries; LMIC: Lower-middle-income countries; UMIC: Upper-middle-income countries; HIC: High-income countries |
||||||||
Discussion
In the age of information overload, where researchers and academics navigate a sea of publishing options, the availability of editorial board information offers a lifeline of credibility. When scholars can easily access details about the experts guiding a journal’s content, it fosters a sense of trust and reliability. Predatory journals, on the other hand, shroud their editorial processes in secrecy, making it difficult for authors to gauge the legitimacy of their platforms. Given the alarming rise of such journals in response to the publish-or-perish pressure [14], it is crucial to uphold established policies for promoting high-quality scientific research. The pressures of the “publish or perish” culture in academia, combined with limited access to resources in LMICs, can sometimes drive researchers towards unethical practices, including plagiarism. Plagiarism, whether intentional or due to lack of proper guidance, poses a significant challenge to maintaining the quality and credibility of scientific research. This is especially relevant in regions where mentorship and training in research ethics may be lacking, further exacerbating the issue. Plagiarism poses a significant challenge in academic publishing, especially for scholars from LICs & LMICs, where pressures to publish, limited resources, and inadequate support systems may contribute to higher risks of unethical practices. Incidents of plagiarism not only tarnish individual academic reputations but also perpetuate the perception that research from these regions is less credible or reliable. This perception can further marginalise LMIC scholars in the global academic community, reinforcing existing disparities in knowledge production and dissemination. The underrepresentation of scholars from LMICs on editorial boards exacerbates this issue, as it may lead to a biased peer review process that fails to account for the unique challenges faced by researchers in these regions. Robust editorial oversight, grounded in ethical guidelines such as those provided by the Committee on Publication Ethics (COPE) [15], is crucial for detecting and preventing plagiarism. To address this, there is a need for increased representation of LMIC scholars on editorial boards, along with targeted education and support initiatives to foster ethical research practices. This approach would help create a more equitable and inclusive academic environment, where all scholars are held to the same standards of integrity and have equal opportunities to contribute to global knowledge.
Some of the key standards and established frameworks widely recognised in academic publishing include the COPE guidelines [15], which emphasise transparency, integrity, and ethical practices in the publication process, and the International Committee of Medical Journal Editors (ICMJE) recommendations [16], which provide guidance on authorship, conflicts of interest, and peer review. Additionally, the Principles of Transparency and Best Practice in Scholarly Publishing [17], jointly established by COPE, the Directory of Open Access Journals (DOAJ), the Open Access Scholarly Publishers Association (OASPA), and the World Association of Medical Editors (WAME), outline standards for editorial board composition, peer review processes, and the avoidance of predatory publishing practices. These frameworks collectively serve as a foundation for maintaining the quality and credibility of scientific research in an era where the proliferation of journals demands rigorous adherence to ethical publishing standards. Adherence to established guidelines enables journals to uphold scientific integrity and contribute to a credible and trustworthy academic environment. In contrast, insufficient transparency may unintentionally expose researchers to publishing challenges that could affect their academic standing. As the number of journals continues to skyrocket, driven by the ever-pressing need to publish frequently, the importance of adhering to established guidelines cannot be overstated. These guidelines serve as the scaffolding upon which the integrity of scientific work rests. By making editorial board information readily available, journals not only support ethical practices but also aid in the cultivation of a vibrant, reputable academic ecosystem.
Uncovering editorial presentations: “The bifurcated reality of skewed views in literature”Our research findings indicate a significant overrepresentation of HICs in the editorial boards of leading Internal medicine journals, a trend consistent with previous studies in related fields such as Saxena et al [12], Dotson [18], and Tutarel [19]. This issue extends beyond clinical medicine, affecting non-clinical and allied healthcare disciplines, including medical education and pharmacology.
A study by Bhaumik and Jagnoor about the examination of global health journals revealed that 26 out of 27 leading international journals were published in HICs [20]. Moreover, only one editor-in-chief hailed from a LMIC, with none from LICs. A staggering 68% of editors were from HICs. While high-income nations often lead in advanced research, this trend persists even in fields that aren’t technology or resource-intensive, raising concerns about the global perspective provided by these journals.
A study by Nafade et al on the editorial board composition of the top 12 global health journals found that only 33% of editors came from LIC and LMICs [21]. This imbalance is exacerbated when considering that a significant portion of the world’s population resides in LMICs like India, Nigeria, and Indonesia. Despite the passage of nearly a decade since some of these studies were conducted, the underrepresentation of other countries on editorial boards remains unchanged. In the context of calls for global equitable representation and inclusivity, especially to avoid making insensitive decisions affecting vulnerable groups, it is evident that editorial boards have yet to adapt to these changing dynamics, highlighting the need for reforms in academia.
Navigating research ethics in a global landscape: Socio-ethical implicationsThe low representation of LMICs and LICs members on the editorial boards of leading academic journals has significant socio-ethical implications. Some of the key points are:
Global knowledge disparitiesThe crux of global knowledge disparities lies, among other factors, in the significant underrepresentation of LICs and LMICs on the editorial boards of influential journals. This fundamental issue perpetuates a cycle of unequal power dynamics in academia. Scholars from HICs wield disproportionate influence over research publication and dissemination, shaping the narrative and priorities of global scientific discourse. This imbalance in representation directly impacts the peer-review process, where diverse perspectives from LMICs and LICs are inadequately considered. As a result, there is a pervasive risk of publication bias against research originating from these regions, hindering the dissemination of valuable insights and impeding scientific progress in underrepresented areas. The consequences of this lack of representation extend beyond academic discourse. It marginalises the voices and research priorities of scholars from LMICs and LICs, limiting their capacity to contribute meaningfully to global knowledge production and dissemination. A seminal study by Larivière et al [22] underscores the long-standing nature of this issue, illuminating the stark global disparities in scientific research and publishing. Efforts to address this disparity are paramount for fostering equity and inclusivity in the global scientific community. By rectifying the underrepresentation of scholars from LMICs and LICs on editorial boards, we can begin to dismantle entrenched power structures and ensure that diverse perspectives are adequately represented in academic decision-making processes. This inclusivity is not just a matter of fairness; it is essential for promoting a more comprehensive and equitable understanding of global issues and advancing scientific progress on a truly global scale. Additionally, diligent monitoring of post-marketing surveillance reports for newly approved drugs in these regions is essential. Initiatives such as the American College of Cardiology Guidelines for hypertension [23], which establish treatment objectives tailored to particular patient cohorts, are a stride in the correct direction.
Obstacles to publishingDisparities in Resource Allocation and Accessibility: The issue of underrepresentation on editorial boards is deeply intertwined with broader challenges in resource allocation and accessibility within the academic research landscape. In LMICs and LICs, the imbalance in representation perpetuates disparities in research funding and opportunities, exacerbating existing inequalities in research infrastructure. In these regions, clinicians often face significant obstacles to engaging in research due to heavy clinical workloads and limited dedicated time for scholarly pursuits. This multifaceted role presents challenges as researchers must balance clinical duties, teaching responsibilities, and research commitments. Due to these challenges, attention to research remains limited, resulting in a dearth of funding opportunities for researchers. Moreover, the underrepresentation on editorial boards of LICs and LMICs exacerbates existing disparities. The lack of representation in these positions often means that research priorities and funding decisions are biased toward the interests of HICs, which further marginalises researchers from less-resourced settings. When editorial boards include members from diverse backgrounds, especially from underrepresented regions, they are more likely to advocate for equitable research priorities and provide a broader range of perspectives that can help address the unique challenges faced by researchers in these settings [24]. The representation on editorial boards can indeed play a crucial role in amplifying the voices of researchers from low-income regions, thereby increasing their access to funding and publication opportunities [25]. Enhanced representation can lead to more equitable decision-making processes, which are essential for addressing the global disparities in research funding and opportunities.
The grants available often fail to adequately address prevalent disease burdens, making impactful research endeavours difficult to pursue [26]. Moreover, the cost associated with publishing in reputable indexed journals presents a significant barrier for researchers in LICs. Article processing charges (APCs) can amount to thousands of dollars, posing a financial burden that is often insurmountable for researchers with limited resources [27]. While some publishers offer fee waivers, these waivers may still be unaffordable for physicians, particularly those working in underserved rural or marginalised areas for low wages. In light of these challenges, researchers in LICs may resort to publishing in predatory journals due to the pressure to publish or perish, compromising the quality and integrity of their research. To address this issue effectively, there is an urgent need for robust and accessible research infrastructure, championed at the policy level. Journal publishers can play a crucial role in addressing these challenges by enhancing fee waiver programmes to enable financially constrained yet scientifically sound researchers to publish in reputable journals. By breaking down traditional cost barriers, publishers can empower physicians and researchers from LICs, ensuring their adequate representation in the scientific community. Our study found that 60% of editorial board members from LICs were affiliated with Cardiovascular Diabetology, while the remaining 40% were associated with the Journal of Hypertension and the Journal of Clinical Hypertension. The relatively higher representation in Cardiovascular Diabetology may be attributed to inclusive policies aimed at encouraging global participation. For instance, the journal offers waivers and discounts on APCs for authors from LICs, reducing financial barriers to publishing [28]. Its open-access model also enhances visibility and accessibility, which is especially beneficial for researchers from LICs who may face difficulties accessing subscription-based journals. For the Journal of Hypertension and the Journal of Clinical Hypertension — also included in our analysis — no specific policies promoting LIC participation were evident in the publicly available information. However, general practices in academic publishing, such as providing discounts or waivers and prioritising open access, could contribute to similar trends. Another notable example of progress in this direction is the recent initiative by the Nature publishing group to offer free article processing for manuscripts accepted in principle from authors in LICs and LMICs. This initiative aims to promote equity and inclusivity in academic publishing, thereby fostering a more representative and diverse scientific community.
Fostering global research equity and collaboration: Addressing language biasWhile efforts are continuously made to enhance global research accessibility, it is crucial to acknowledge that a significant proportion of research manuscripts will continue to be in English. In fields like medical research, which prioritise patient-centricity, substantial work is conducted in regional and national languages. Tasks such as obtaining informed consent, patient counselling, and data collection via validated questionnaires are performed in the language most comfortable for patients. Despite initiatives like Open Access Week striving to facilitate the free sharing of research findings, language barriers diminish their envisioned impact, as many patients are not proficient in English. Even among researchers conducting systematic reviews and meta-analyses, the “Tower of Babel” bias often arises, leading to data from papers published in regional languages being difficult to extract and, consequently, excluded [29]. This exclusion reduces the influence of such research and discourages researchers from publishing in regional languages, contributing to the decline in non-English papers in medical literature [30].
As a consequence, regional research is under-referenced, creating a cycle where physicians comfortable with these languages must invest in costly language editing services to ensure their research reaches the intended audience. A more practical alternative would be for them to publish their work in their native language, aligning with both the authors’ and patients’ preferences. Journals could explore implementing a multilingual publishing model, featuring articles in various languages within each issue. Innovative solutions for effective translation, surpassing automated services’ placeholder translations, could enhance visibility and citations. This would genuinely fulfil the promise of “open access” by ensuring readers can access and benefit from research regardless of the language in which it was originally published. Increasing representation from LMICs and LICs can foster stronger international collaborations, encouraging knowledge exchange and cooperation across borders [29].
Disincentive for local research and limitation of innovation: a dual challengeIn LICs, the pursuit of scientific research and innovation faces a daunting dual challenge characterised by a significant disincentive for local research and a constraining limitation of innovation. These nations, often burdened by resource constraints, infrastructure deficiencies, and healthcare disparities, find themselves grappling with a critical need to bolster their scientific capabilities while simultaneously confronting barriers that hinder progress. The disincentive for local research, often driven by limited funding opportunities and a reliance on external research agendas, is compounded by limited innovation stemming from a lack of access to cutting-edge technology and knowledge diffusion. Prominent journals consistently feature articles that garner the highest citation counts, yet they predominantly originate from HICs, exacerbating the well-documented 10/90 gap in the field of medical research (Global Forum for Health Research) [31]. This observation aligns with Bradford’s Law of Dispersion, a renowned principle indicating that a handful of select journals collectively contribute the majority of citations within a given subject area [32]. These obstacles hamper both indigenous research growth and innovative solutions for healthcare, economic, and societal challenges in LICs. Addressing these intertwined challenges demands a multifaceted approach to catalyse research and innovation ecosystems, promoting sustainable development and global collaboration. A survey involving corresponding authors of articles from 131 Medline-indexed pharmacology journals revealed that 40% of respondents believed editors and reviewers held doubts about research from LIC and LMICs, extending these doubts to research methodology and data collection [4]. This discouragement may lead researchers in LMICs and LICs to refrain from pursuing research or publishing in international journals, fostering distrust in the academic publishing system due to perceived bias and exclusion. Such underrepresentation stifles innovation, as research from these regions often offers unique perspectives and solutions that require diverse editorial board input.
Impact on policy and practiceLeading journals wield substantial influence over policy and practice in various fields. However, a notable concern arises when the voices of LMICs and LICs are underrepresented on the editorial boards of these influential publications. A study by Rawat et al [33] showed that the majority of editorial board members of leading obstetrics and gynaecology journals were from HICs and only a meagre proportion of them were from LIC and LMIC. Another study by Melhem et al [34] reported that the editorial staff in leading biomedical journals was largely composed of individuals affiliated to HICs in North America and Europe. This underrepresentation can potentially lead to research outcomes that fall short in effectively informing policies and interventions within these nations, thereby raising critical questions about the inclusivity and global relevance of the research ecosystem. In this context, examining the impact of diverse editorial perspectives on policy and practice becomes a matter of paramount importance.
In summary, the low representation of LMIC and LIC members on the editorial boards of leading journals not only perpetuates inequality in the academic publishing landscape but also has far-reaching socio-ethical implications, restricting production, policy development, and the overall progress of science and research on a global scale. Addressing this issue is crucial for creating a more equitable and inclusive scholarly ecosystem.
Recommendations for improvementTo improve the situation of low representation of LMIC and LIC members on the editorial boards of leading journals, various steps can be taken. Here are some recommendations:
Fostering inclusivity and collaboration in global researchTo enhance global research inclusivity, establishing diversity initiatives within journal editorial boards is crucial. Setting clear diversity targets and tracking progress is essential, alongside fostering international collaboration through partnerships with institutions in LMICs & LICs. Physicians from LICs and LMICs may struggle to join academic editorial boards due to resource and language barriers. To overcome this, support should be given to interest groups and research bodies representing specific subsets. For instance, clinical groups such as British Association of Physicians of Indian Origin (BAPIO) can facilitate fair representation, extending this to gender, race, ethnicity, and other socio-demographic factors [35, 36]. This promotes a more inclusive academia and diverse editorial perspectives. These partnerships can lead to joint editorial efforts aimed at increasing diversity and inclusivity in research dissemination, ensuring that a broader array of voices and perspectives are heard. Additionally, it is imperative to consider the role of unpaid peer review in the composition of editorial boards, especially with regard to the under-resourcing in LICs. By addressing the issue of unpaid peer review and advocating for fair compensation, we can potentially enhance the representation of researchers from LICs on editorial boards. Paid peer review can serve as a pathway for individuals in LICs to gain visibility and recognition, ultimately increasing their likelihood of receiving editorial invitations. Furthermore, collaborative research initiatives should be promoted, transcending borders and involving researchers from both HICs and LICs. This approach encourages a more inclusive and holistic approach to knowledge creation, breaking down barriers and harnessing the collective expertise of diverse research communities. Through these concerted efforts, the global research community can work together to bridge gaps, promote diversity, and advance equitable access to knowledge and opportunities for all.
Mentorship programmes and capacity building opportunitiesTo promote diversity and inclusivity within journal editorial boards and empower researchers from LMICs and LICs, the establishment of mentorship programmes is essential. These programmes can pair junior researchers from LMICs and LICs with experienced editorial board members, providing them with valuable guidance and support. Through mentorship, these aspiring board members can gain insights into the editorial process and develop their skills. Additionally, offering training and capacity-building opportunities is crucial. By providing training in peer review and editorial work, potential board members from underrepresented regions can enhance their expertise and competencies. These programmes help bridge the knowledge gap and empower individuals to actively contribute to the editorial process, ensuring a more equitable representation of diverse perspectives in the realm of academic publishing.
Nurturing transparency and diversity in editorial appointmentsAppointing members to editorial boards often lacks transparency, leaving room for questions regarding the process. Many journals accept applications for board positions on an ongoing basis and some board members hold honorary roles across multiple journals. While not inherently problematic, this approach places significant emphasis on an editor’s academic reputation, which includes factors like references, citations, and personal achievements. This emphasis creates a subjective process that can be scrutinised. Unfortunately, most journal websites provide little to no information about the timing of board renewals or notifications of vacant positions. Often, board appointments occur internally within academic circles, excluding external applicants and causing them to miss opportunities. Furthermore, the majority of journals do not share statistics regarding the number of applications received or their appointment procedures, which hampers transparency. To address these concerns, Teixeira da Silva and Al-Khatib [37] suggests that journals adopt more transparent and inclusive practices by regularly publishing appointment statistics, similar to the transparency seen in residency match or grant application processes. Additionally, they recommend that journals establish and publicly share clear criteria for board appointments, ensuring that these criteria are accessible to a broader range of potential applicants. Implementing these suggestions would enhance transparency and improve accountability within the editorial board selection process.
Actively recruiting qualified candidates from LMICs and LICs fosters inclusivity, facilitated by collaboration with regional institutions. Regular evaluations of editorial boards, focusing on composition and performance, rectify biases and maintain diversity and high publishing standards.
By implementing these recommendations, journals can take concrete steps to address the underrepresentation issue and promote a more equitable and inclusive scholarly publishing ecosystem that benefits researchers from all regions of the world.
Limitations
One limitation of this study pertains to its use of income groups as a method for assessing international representation equitability. Some argue that income classifications have become somewhat arbitrary and less relevant in today’s rapidly evolving global [38]. However, due to the scarcity of comparable global data for other suitable social indicators, income group classification remains a reasonably accurate reflection of national development characteristics. Another limitation is that while our study is primarily focused on geographic and economic diversity, the lack of accessible gender data underscores the broader issue of transparency in editorial board composition. Future research should consider the inclusion of gender as a key dimension of diversity, provided that such data is made available. Additionally, this study did not consider the hierarchy within the editorial boards of leading journals. Future research could explore the distribution of the countries of origin among editor-in-chief, assistant editors, and section editors, as each of them wields a distinct influence on publication decisions.
Analysing authorship patterns in these journals could shed light on regions that still lack the equitable representation necessary for shaping effective global policies. This pertains not only to Internal medicine but also extends to other medical disciplines, highlighting the importance of fair representation for high-interest, high-power stakeholders.
Conclusion
LICs and LMICs face significant underrepresentation on the editorial boards of internal medicine journals. This lack of diversity in medical research and decision-making poses a serious risk to a substantial portion of the world’s population. To address this issue, it is imperative to initiate large-scale international collaborations and prioritise the establishment of suitable resources that promote equitable participation in research.
Addressing this issue requires a multifaceted approach, including large-scale international collaborations and the establishment of resources that promote equitable participation in research. However, the implications of this study extend beyond internal medicine journals. The recommendations provided here are relevant to journals across all scientific disciplines, from the natural and social sciences to the humanities. By implementing these strategies, journals can contribute to a more diverse and inclusive editorial landscape. By increasing the proportion of editors from underrepresented regions, journals not only enhance visibility and inclusion but also enrich the global research community. This approach fosters a more equitable and inclusive scientific landscape, ensuring that research and medical advancements benefit all populations.
Authors: Jasmeet Singh (corresponding author — meetjas290101@gmail.com, https://orcid.org/0009-0003-8465-8984), University college of medical sciences and GTB hospital, New Delhi-110095, INDIA; Pratyush Kumar (pratyushkumar9958@gmail.com, https://orcid.org/0000-0002-5275-1952), Dr Baba Saheb Ambedkar Medical College and Hospital, New Delhi, INDIA; Abhishek Kumar (kra09757@gmail.com, https://orcid.org/0000-0003-4402-3856), Dr Baba Saheb Ambedkar Medical College and Hospital, New Delhi, INDIA.
Authors’ contribution: JS: conceptualising, designing, material preparation, formulated the outline and key arguments, final manuscript review; PK: conceptualising, designing, data analysis, final manuscript review; AK: conceptualising, designing, data collection, final manuscript review.
Conflict of Interest: None declared Funding: None
Ethics approval: Not applicable
Data sharing: Data not made available in the public domain. Please contact the corresponding author for access to raw data.
To cite: Singh J, Kumar P, Kumar A. Global disparities and data transparency in editorial boards of prominent Internal medicine journals including allied super specialities: A wake-up call. Indian J Med Ethics. 2025 Oct-Dec; 10(4) NS: 278-287. DOI: 10.20529/IJME.2025.045
Submission received: May 31, 2024
Submission accepted: September 27, 2024
Published online first: June 3, 2025.
Manuscript Editor: Sunu C Thomas
Peer Reviewers: Three anonymous reviewers
Copyright and license
©Indian Journal of Medical Ethics 2025: Open Access and Distributed under the Creative Commons license (CC BY-NC-ND 4.0), which permits only noncommercial and non-modified sharing in any medium, provided the original author(s) and source are credited.
References
- World Bank. World Bank country and lending groups. 2023 [cited 2024 Sept 7]. Available From: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups
- Aluede EE, Phillips J, Bleyer J, Jergesen HE, Coughlin R. Representation of developing countries in orthopaedic journals: a survey of four influential orthopaedic journals. Clinical Orthopaedics and Related Research. 2012;470(8):2313–2318. https://doi.org/10.1007/s11999-012-2377-5
- Rohra DK. Representation of less-developed countries in Pharmacology journals: an online survey of corresponding authors. BMC Medical Research Methodology. 2011;11:60. https://doi.org/10.1186/1471-2288-11-60
- Saxena S, Paraje G, Sharan P. The 10/90 divide in mental health research: Trends over a 10-year period. British Journal of Psychiatry. 2006;188(1):81–82. https://doi.org/10.1192/bjp.bp.105.011221
- Hamadeh, Nada, Catherine Van Rompaey, Eric Metreau, and Shwetha Grace Eapen. 2022. New World Bank country classifications by income level: 2022-2023. World Bank Blogs,1 July 2022[cited 2024 Sept 7]. Available from: https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2022-2023
- Modlin CE, Deng Q, Benkeser D, Mulate YW, Aseffa A, Waller L, Powell KR, Kempker RR. Authorship trends in infectious diseases society of America affiliated journal articles conducted in low-income countries, 1998-2018. PLOS Glob Public Health. 2022 Jun 10;2(6):e0000275. https://doi.org/10.1371/journal.pgph.0000275
- Horton R. North and South: bridging the information gap. Lancet. 2000 Jun 24;355(9222):2231-6. https://doi.org/10.1016/s0140-6736(00)02414-4
- Sumathipala A, Siribaddana S, Patel V. Under-representation of developing countries in the research literature: ethical issues arising from a survey of five leading medical journals. BMC Medical Ethics. 2004 Oct 4; 5 (1): E5. https://doi.org/10.1186/1472-6939-5-5
- Igoumenou A, Ebmeier K, Roberts N, Fazel S. Geographic trends of scientific output and citation practices in psychiatry. BMC Psychiatry. 2014 Dec 6;14:332. https://doi.org/10.1186/s12888-014-0332-6
- Mari JJ, Patel V, Kieling C, Razzouk D, Tyrer P, Herrman H. The 5/95 gap in the indexation of psychiatric journals of low- and middle-income countries. Acta Psychiatr Scand. 2010 Feb;121(2):152-6. https://doi.org/10.1111/j.1600-0447.2009.01476.x
- Harris CA, Banerjee T, Cramer M, Manz S, Ward ST, Dimick J, Telem DA. Editorial (Spring) Board? Gender Composition in High-impact General Surgery Journals Over 20 Years. Ann Surg. 2019 Mar;269(3):582-588. https://doi.org/10.1097/sla.0000000000002667
- Saxena S, Levav I, Maulik P, Saraceno B. How international are the editorial boards of leading psychiatry journals? Lancet. 2003 Feb 15;361(9357):609. https://doi.org/10.1016/s0140-6736(03)12528-7
- Falagas ME, Kouranos VD, Arencibia-Jorge R, Karageorgopoulos DE. Comparison of SCImago journal rank indicator with journal impact factor. FASEB J. 2008 Aug;22(8):2623-8. https://doi.org/10.1096/fj.08-107938
- Elmore SA, Weston EH. Predatory Journals: What They Are and How to Avoid Them. Toxicol Pathol. 2020 Jun;48(4):607-610. https://doi.org/10.1177/0192623320920209
- Committee on Publication Ethics. COPE Core Practices. 2023 [cited 2024 Sept 7]. Available from: https://publicationethics.org/core-practices
- International Committee of Medical Journal Editors. Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals. 2023 [cited 2024 Sept 7]. Available from: http://www.icmje.org/recommendations/
- Directory of Open Access Journals. Principles of Transparency and Best Practice in Scholarly Publishing. 2024 [cited 2024 Sept 7]. Available from: https://doaj.org/apply/transparency
- Dotson B. Geographical composition of the editorial boards of leading pharmacy journals. Am J Pharm Educ. 2012 Oct 12;76(8):160. https://doi.org/10.5688/ajpe768160
- Tutarel O. Composition of the editorial boards of leading medical education journals. BMC Med Res Methodol. 2004 Jan 20;4:3. https://doi.org/10.1186/1471-2288-4-3
- Bhaumik S, Jagnoor J. Diversity in the editorial boards of global health journals. BMJ Glob Health. 2019 Oct 18;4(5):e001909. https://doi.org/10.1136/bmjgh-2019-001909
- Nafade V, Sen P, Pai M. Global health journals need to address equity, diversity and inclusion. BMJ Glob Health. 2019 Oct 18;4(5):e002018. https://doi.org/10.1136/bmjgh-2019-002018
- Larivière V, Ni C, Gingras Y, Cronin B, Sugimoto CR. Bibliometrics: global gender disparities in science. Nature. 2013 Dec 12;504(7479):211-3. https://doi.org/10.1038/504211a
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018 May 15;71(19):e127-e248. https://doi.org/10.1016/j.jacc.2017.11.006
- Biswas J, Dhali A, Rathna RB, D’Souza C. Authorship diversity in hematology-related Cochrane systematic reviews: Inequities in global representation. Res Pract Thromb Haemost. 2022 Aug 16;6(6):e12778. https://doi.org/10.1002/rth2.12778
- Gasparyan AY, Ayvazyan L, Blackmore H, Kitas GD. Writing a narrative biomedical review: considerations for authors, peer reviewers, and editors. Rheumatol Int. 2011 Nov;31(11):1409-17. https://doi.org/10.1007/s00296-011-1999-3
- Dandona L, Dandona R, Kumar GA, Cowling K, Titus P, Katoch VM, Swaminathan S. Mapping of health research funding in India. Natl Med J India. 2017 Nov-Dec;30(6):309-316. https://doi.org/10.4103/0970-258x.239069
- Solomon D, Björk BC. Article processing charges for open access publication-the situation for research intensive universities in the USA and Canada. PeerJ. 2016 Jul 21;4:e2264. https://doi.org/10.7717/peerj.2264
- Cardiovascular Diabetology. About this journal. 2024 [cited 2024 Sept 7]. Available from: https://cardiab.biomedcentral.com/about
- Fovet T, Horn M, Lancelevee C, Thomas P, Amad A. Language bias in forensic psychiatry research: the tower of Babel problem: Comment on ‘Potential language bias in systematic reviews on the use of coercion in psychiatry’. Acta Psychiatr Scand. 2020 Sep;142(3):257-258. https://doi.org/10.1111/acps.13227
- Šember M, Petrak J. Radovi Doktorskih Kandidata S Medicinskog Fakulteta Sveučilišta U Zagrebu U Hrvatskim Časopisima. [Publications in the Croatian Medical Journals by doctoral candidates at University of Zagreb School of Medicine]. Liječnički vjesnik. 2014[cited 2024 Sept 7];136(1-2). Available from: https://hrcak.srce.hr/172577
- Global Forum for Health Research, 2000. The 10/90 (ten ninety) report on health research 2001-2002. Geneva: Global Forum for Health Research. [cited 2024 Sept 7]. Available from: https://iris.who.int/handle/10665/44385
- Cascajares M, Alcayde A, Salmerón-Manzano E, Manzano-Agugliaro F. The Bibliometric Literature on Scopus and WoS: The Medicine and Environmental Sciences Categories as Case of Study. Int J Environ Res Public Health. 2021 May 29;18(11):5851. https://doi.org/10.3390/ijerph18115851
- Rawat S, Mathe P, Unnithan VB, Kumar P, Abhishek K, Praveen N, Guleria K. Poor Representation of Developing Countries in Editorial Boards of Leading Obstetrics and Gynaecology Journals. Asian Bioeth Rev. 2023 Feb 7;15(3):241-258. https://doi.org/10.1007/s41649-023-00241-w
- Melhem G, Rees CA, Sunguya BF, Ali M, Kurpad A, Duggan CP. Association of International Editorial Staff With Published Articles From Low- and Middle-Income Countries. JAMA Netw Open. 2022 May 2;5(5):e2213269. https://doi.org/10.1001/jamanetworkopen.2022.13269
- Anaesthesia Journal Editorial Board Diversity and Representation Study Group. Trends in country and gender representation on editorial boards in anaesthesia journals: a pooled cross-sectional analysis. Anaesthesia. 2022 Sep;77(9):981-990. https://doi.org/10.1111/anae.15733
- Leung KK, Jawaid N, Bollegala N. Gender differences in gastroenterology and hepatology authorship and editorial boards. Gastrointest Endosc. 2021 Oct;94(4):713-723. https://doi.org/10.1016/j.gie.2021.05.019
- Teixeira da Silva JA, Al-Khatib A. How are Editors Selected, Recruited and Approved? Sci Eng Ethics. 2017 Dec;23(6):1801-1804. https://doi.org/10.1007/s11948-016-9821-y
- Beer Prydz, Espen, and Divyanshi Wadhwa. 2019. Classifying countries by income. World Bank, 2019 September 9 [cited 2024 Sept 7]. Available from: https://datatopics.worldbank.org/world-development-indicators/stories/the-classification-of-countries-by-income.html