This article highlights the importance of advance care planning (ACP) in good end-of-life care (EOLC). The judgement by the Supreme Court of India legalised Advance Medical Directives in 2018 and in January 2023, amended the procedure to make it easier. The article describes the advantages of ACP, the numerous ethical dilemmas at the end of life that it seeks to address and avoid, the latest legal procedure, the barriers, the need for awareness among healthcare providers, legal professionals as well as the public, and the need for legislation to translate the law into action. Educating citizens about their right to choose the kind of care they want at the end of life, including the right to refuse treatment, is the moral and ethical duty of all health professionals. Making death literacy and ACP a part of a public health initiative would be a major step towards meeting the obligations reflected in the World Health Organization guidelines and National Health Policy 2017, which envisage palliative care and EOLC as an integral part of Universal Health Coverage, requiring support from the government as well as the participation of civil society.
Keywords: advance care planning, living will, palliative care, end of life care, public health, death literacy
India has been consistently ranked amongst the world’s worst countries to die in, ranking 40th out of 40 countries in 2010, 67th out of 85 in 2015 and 59th out of 81 in 2021 in the Outcomes of Quality of Death Index Report [1, 2, 3]. The causes for such low ranking include lack of access to palliative care (PC), cultural taboos deterring discussions on death and dying, and lack of attention to care as one of the aims of management with overemphasis on cure. Over the last century, huge advances in diagnostics and therapeutics have diminished the importance of prognostication [4] and medicalised death, denuding it of social and spiritual meaning [5].
Palliative care is defined as “an approach that improves the quality of life of patients and that of their families who are facing challenges associated with life limiting illness, whether physical, psychological, social or spiritual” [6]. It includes, but is not limited to End-of-life care (EOLC). Till recently, PC has not been part of undergraduate medical education in India. Therefore, the majority of doctors and healthcare professionals have not been trained to address the multi-dimensional issues arising during terminal illness and death. Lack of clarity on legal guidelines for EOLC especially the withholding and withdrawal of inappropriate, aggressive treatment gave rise to the fear of being accused of sub-optimal treatment and possible criminal liability, leading to inappropriately aggressive treatment and ICU care, even when there is no reasonable hope of cure or treatment becomes burdensome [7, 8].
In India, prolonged and futile treatment leads to considerable financial burdens for patients and families. High out-of-pocket health expenditure impoverishes almost 55 million Indians annually, with over 17% households incurring catastrophic levels of health expenditure [9]. Non-availability of EOLC and rising costs force up to 78% Indian patients to leave hospitals against medical advice — apparently on their own but often with tacit encouragement by the doctors — without receiving symptom control, EOLC guidance/support, and dying in distress and pain [7].
The World Health Organization (WHO) recognises PC as an ethical responsibility as part of universal health coverage. This requires appropriate policy support, adequate drug availability, education of policymakers, health workers and the public, and integration of services at all levels of healthcare [10]. Palliative care is one of the components of India’s National Health Policy, 2017 which aims at universal health coverage [11]. The challenge is to make PC viable in our fragmented healthcare systems. Advance care planning has been found to be an important public health strategy to increase the public’s acceptance and visibility of PC. ACP thus becomes an important public health initiative which can help improve EOLC [12] through the process of informed, joint decision-making with the consensus of patients and caregivers within an ethical framework.
One of the pillars of palliative care is joint decision-making with the patient and caregiver after giving them honest information regarding the illness and the prognosis, respecting their choices and providing care at the place of the patient’s choice, allowing them to spend their time as and where they wish. This is important from the viewpoint of respecting their autonomy as well as providing ethically sound treatment choices. Advance care planning or “Living Will” is a tool that allows patients to communicate their choices, making it easier for both caregivers and healthcare professionals to take decisions that honour their wishes.
ACP is defined as the process that “Enables individuals who have decisional capacity to identify their values, reflect upon the meanings and consequences of serious illness scenarios, define goals and preferences for future medical treatment and care, and discuss these with family and health-care providers. It addresses individuals’ concerns across the physical, psychological, social, and spiritual domains, encouraging them to identify a personal representative and to record and regularly review any preferences, so that these can be taken into account should they, at some point, be unable to make their own decisions.” [12] It is a process that involves informing individuals about the possibilities or current diagnoses, prognoses, types of treatment available including life-sustaining treatment, eliciting the personal cultural and spiritual outlook on what is meaningful to them, their perception of a good death, treatment options they would or would not want in case of a life-limiting illness, appointment of surrogates who can take decisions on their behalf if they are not in a condition to do so, and sharing these preferences with families and healthcare providers (HCPs). ACP takes place over time and requires a number of conversations with the patient and caregivers [12, 13]. The process of ACP (Table 1) [14] can be done for healthy adults at any stage of life, with an individualised approach but its contents could be more targeted for the elderly or those with worsening health. It is applicable across a variety of patient populations in different healthcare and cultural settings. Ideally, ACP must be proactive, appropriately timed, and integrated into routine care [12, 15]. Standardised, structured, locally relevant conversation guidelines are helpful in different patient groups [1]. These include exploration of patients’ perspectives on illness, meaning of a good life, end-of-life issues, and decision-making and ensuring understanding of key concepts [16, 17, 18, 19].
Table.1. Process of ACP. [14]
STEPS |
Activities by healthcare workers or trained facilitators |
Sample Conversations |
| INITIATE |
o Identify beneficiaries o Introduce and normalise the ACP concept o Check for existing AMD, is it valid? |
We encourage all our patients to think about planning for the future? What do you understand/have been told about your illness? Any questions you still have? When you think about the future, are there things you worry about…hope for? |
| EDUCATE |
o Explain concept, advantages and limitations, available resources and documents o Encourage the selection of surrogate decision maker/s o Check perceptions of CPR, ICU care and outcomes |
Who would you want to speak for you when you cannot? You can hope for the best but you must plan for the rest. A heart attack means that the heart has stopped and has to be restarted. In someone who is dying, when the heart stops, it cannot be restarted. |
| DISCUSSION |
o Request the presence of the surrogate decision maker o Explore values in relation to death/dying, dependence, dignity, religious background, finances o Elicit goals of care for longevity/survival, maintenance of function, suffering/comfort o Recommend treatment plans (optional) in line with values and goals of care |
What would you like to do if time ran short? What trade- offs are you willing to make for added time? How much suffering would be acceptable for the sake of added time? May I suggest a treatment plan that allows you to work toward your goals. I would recommend… |
| DOCUMENT |
o Discussions to be documented in medical records o Ensure that completed AMD copies are availa ble with all concerned (patient, surrogate/family, HCP), subject to privacy concerns |
|
| SUMMARIZE
AND CLOSE |
o Use standard closing phrases, checking for concerns o Revisit and review |
I know this has been a lot to discuss…You are brave to talk about this… I will be with you at every step. If you don’t mind, I will check in with you once a year about these documents to see that they still fit your needs and wishes. |
The patient’s wishes are put on record in the form of legal documents called Advance Directives (ADs). The Indian Council of Medical Research (ICMR) defines AD as “a statement made by a person with decision making capacity stating his/her wishes regarding how to be treated or not treated at a stage when s/he loses such capacity” and a surrogate decision maker as a “person or persons other than the health care providers who is/are accepted as the representatives of the patient’s best interests, who will make decisions on behalf of the patient when the patient loses decision making capacity.” [20] AD, therefore, is a legal document and thus different from ACP — which is the whole process involving information, communication, eliciting and recording wishes. ADs are thus only one part of the bigger process of ACP [1]. In 2018, the Supreme Court (SC) of India, in response to a public interest litigation filed by the NGO, Common Cause, recognised citizens’ right to execute ADs, including the right to refuse treatment if terminally ill or in a persistent vegetative state [7, 21]. However, the procedure prescribed was cumbersome enough to be practically impossible [7, 22, 23]. Thereafter, an application filed by the Indian Society of Critical Care Medicine and Common Cause to simplify the process was considered favourably by the SC and revised directions pronounced in January, 2023 [23]. Any adult with decision-making capacity can prepare a legally valid AD, which must be signed only by two independent witnesses and either be notarised or attested by a gazetted officer. There is an easier two-tier process for withdrawing/withholding care in hospitalised patients who do not have capacity, irrespective of an AD or nominated surrogate being available. Two medical boards need to be set up by the hospital/institution to take the decision. The district magistrate, needs only to be “intimated” — no authorisation is needed. The AD can be changed in writing or revoked at any time. If changed more than once, the most recently signed AD is valid and given effect. This provides guidance and moral authority to families too. No hospital or doctor is liable in civil/criminal proceedings for obeying an AD. Doctors citing conscientious objection on religious grounds are exempted, but hospitals are obliged to honour it [23].
Changing values and preferences over time require documents to be updated regularly [12, 13] although the data suggests that completion of ADs is associated with stable preferences [13]. Different models for implementation are available: in-clinic/hospital discussion with physicians, facilitated conversations with trained facilitators at home or elsewhere, and community wide dissemination preferably by peer educators. ACP campaigns involve raising awareness, advocacy, monitoring policy implementation or acting as pressure groups to influence political opinion [12]. Using tools and aids for recurrent discussions with all stakeholders, training in communication skills, delegation of some tasks to team members and including volunteers, community members and NGOs can overcome some issues like barriers due to language, lack of education or paucity of time in the public system and language, education or patriarchal practise in the Indian set up. Studies suggest that discussing ACP and EOLC with doctors may be more helpful than just completing a legal document. Documentation should not be so complicated as to discourage conversations [20].
ACP has been helpful in navigating many of the ethical dilemmas inherent in EOLC all over the world [10,12]. In the Indian context, the legal haze surrounding end-of-life policy and decisions has been clarified by the SC, making it easier for healthcare workers to support patient autonomy, in cases where the families’ preference is at variance with the patient or where families pressurise healthcare workers to “do everything possible”; when factors other than the patients’ best interest dictate continuation of futile, inappropriate aggressive treatment/ICU care and when there is disagreement between teams or families. ACP eases family concerns during withdrawal/withholding of life-supporting treatment. It can cover consent for organ donation, including the nascent process of donation after cardiac death. It becomes especially relevant in serious, progressive conditions having high prognostic uncertainty where decisional capacity may be lost. It has been shown in earlier studies in the West to enable more AD completion, alignment of care with patient’s preferences, decreased emergency and unwanted hospitalisation, better communication between patients, families and providers [12, 24, 25, 26, increased palliative care utilisation, greater optimism among beneficiaries [27, 28], and less moral distress among HCPs [24]. In the Netherlands, a 2014 systemic review where the majority of studies were from the USA, found ACP effective in decreasing life-sustaining treatment, increasing use of hospice and palliative care and preventing hospitalisation. Complex ACP interventions seemed to increase compliance with patients’ end-of-life wishes [26].
The legal position is now unambiguous and the right of every Indian citizen to a pain-free and dignified death has been spelt out. What now needs to be done is to improve death literacy, “a set of knowledge, skills, experiences, attitudes and behaviours that help individuals and communities deal with death, dying and loss.” [29] Educating the public has an important role in improving death literacy within the public health approach to palliative care [27]. Death literacy is high when people and the community are well informed about the local death system and can translate it into practice. In public health, it is considered an outcome of people’s experiences of and learnings about, death and dying — a resource that strengthens their ability to plan, deal with and care for the dying, support others who might be facing similar situations related to death and dying — benefiting the community as a whole [28, 29, 30].
It is thus befitting its role as the National body for PC in India, that the Indian Association of Palliative Care (IAPC) plans to take ownership of ACP and lead the country in planning and implementation through:
• An awareness campaign with live webinars in all major Indian languages, recordings of which, along-with appropriate information, resources and a dedicated team to answer queries will be available on its website.
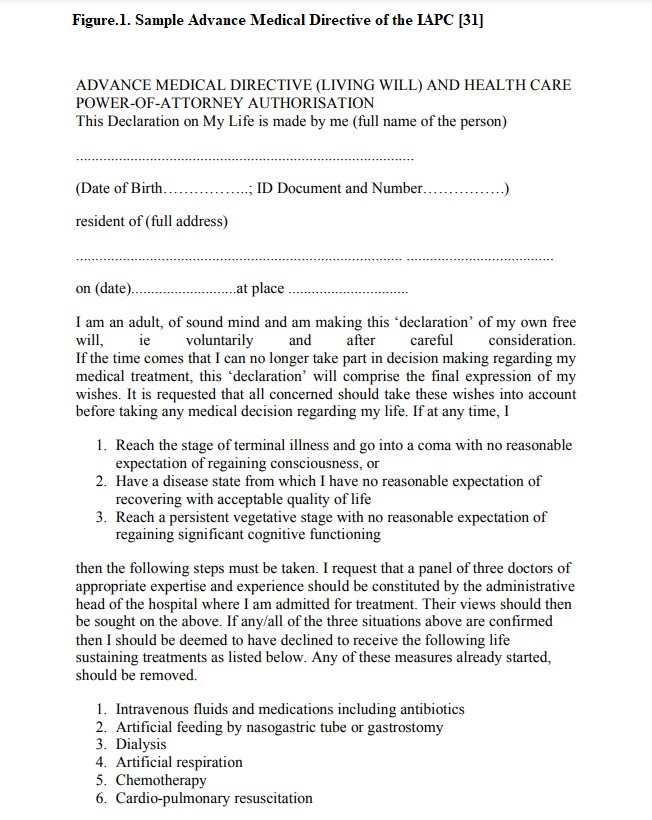
• Developing a model Advance Medical Directive (See Figure 1, available online only) [31].
• Facilitator training and support in vernacular languages through international collaborations.
• Community capacity building by a dedicated not-for-profit organisation. • Focus group discussions to understand the needs of various ethno-religious groups for designing appropriate material.
• Reaching out to faith-based organisations and leaders to introduce it to their own communities.
• Civil society playing a major role in both advocacy and partnership, to provide administrative and financial support for publicity campaigns, to develop culturally relevant educational material and as coordinators.
• Advocacy with policy-makers and legislators for formulating laws to implement the SC judgment. A central Act would be easier to implement across the country and ensure uniformity of documentation too.
It is thus an ethical obligation for us, as physicians, to take this important issue forward and advocate for ACP and good EOLC in our own practice, in our organisations and in our communities, so that every Indian citizen can benefit from ACP, get access to PC and be able to exercise their right to a peaceful, pain-free and dignified end, at the place and in the manner of their own choice.
EOLC involves complex medical decisions that require repeated conversations within an ethical framework for enabling autonomy through joint decision-making. ACP is a process that can help in avoiding inappropriate treatment and referrals which cause significant harm through pain and distress to patients and a psycho-social-financial burden for families. The beneficence that it offers to patients in terms of respecting choices, to communities in terms of improved quality of both life and death, and to the nation in terms of socially just distribution of healthcare resources, prevention of financial burden and better indicators of health-related suffering, are well-worth the effort required for improving death literacy in the providers and public. The recent Supreme Court judgment has given this legal sanction. Now, it is for the medical profession to embrace the concept of ACP for better EOLC, make improving death literacy a public health priority, and take it up as a moral and ethical duty to make living and dying with dignity in India a possibility in the years ahead.
“We will die in the system we create.” Dr Laurel Herbst [32]
{kind=link}