ARTICLES
The process of justifying assisted reproductive technologies in Iran
Ehsan Shamsi Gooshki, Neda Allahbedashti
DOI: https://doi.org/10.20529/IJME.2015.027
Abstract
Infertility is medically defined as one year of unprotected intercourse that does not result in pregnancy. Infertility is a noticeable medical problem in Iran, and about a quarter of Iranian couples experience primary infertility at some point in their lives. Since having children is a basic social value in Iran, infertility has an adverse effect on the health of the couple and affects their well-being. The various methods of assisting infertile couples raise several ethical questions and touch upon certain sensitive points. Although the present Iranian legislative system, which is based on the Shi’a school of Islam, has legalised some aspects of assisted reproductive technologies (ARTs), given the absence of a general officially ratified act (official pathway), such medical interventions are usually justified through a fatwa system (non-official pathway). Officially registered married couples can access almost all ART methods, including third-party gamete donation, if they use such pathways. The process of justifying ART interventions generally began when in vitro fertilisation was given the nod and later, Ayatollah Khamenei (the political-religious leader of the country) issued a fatwa which permitted gamete donation by third parties. This open juristic approach paved the way for the ratification of the Embryo Donation to Infertile Spouses Act in 2003.
Introduction
Traditionally, having children is one of the basic values cherished by Iranian society (1). Infertility is usually defined as one year of unprotected intercourse that does not result in pregnancy (2). Infertile couples run a relatively high risk of suffering from health problems and they have a lower quality of life due to the stigma of being childless. To solve the problem, they often try out traditional methods that may not be safe and medically approved. Infertile women live in constant fear of being abandoned, as polygyny is accepted in Iranian society (3). Infertility also adversely affects the emotional well-being of the couple, particularly the woman (4, 5). In Iran, infertility is a noticeable medical problem, with about a quarter of couples experiencing primary infertility at some point in their lives (6). Although different rates for prevalence of infertility have been reported in some parts of the country between 2002 and 2008 (7, 8, 9), more recent studies have claimed the prevalence rate of 20% for primary infertility in Iran (10).
As in -many developed countries, 2–4% of all children in Iran are born with the help of assisted reproduction technologies (ARTs) (11). Given the high prevalence of infertility and the cultural resistance to adoption (12), public demand for the development of ARTs within the country has been increasing. As a result of this overwhelming demand, the health system is being pushed to provide more appropriate services, as well as seek jurisprudential and legal legitimacy from the religious authorities and legislative system, which is based on Shi’a jurisprudence.
The first case of in vitro fertilisation (IVF), in 1978 (13, 14) gave rise to ethical and legal debates on the use of ARTs (15). In 1990, the country’s first IVF baby was born (16). The use of this procedure increased dramatically from then on (17). At present, there are no legal or religious barriers to the use of various ARTs (18). When it comes to these technologies, Iran is undoubtedly the leading country in the Muslim world (19). Various ART methods are used in Iran’s ART centres, which are supervised by the Ministry of Health and Medical Education (MOHME) (20).
Today, Iran is the only country that has a legal system based on the Shi’a school of Islam. While few laws exclusively on ethical standards in biomedical practice have been ratified, other more general laws, such as the Constitution of the Islamic Republic of Iran (21) (articles 3, 21, 29, 43) and Public Insurance Law (22), take note of ethical issues at a basic level. These laws emphasise mainly the principles of justice. Mention must also be made of Iran’s Civil Code, which names compatibility with moral norms as a precondition for making contracts and taking actions (23). Although these legal requirements are very general and cannot be considered to be serious guarantees for ethical practice in the field of biomedicine, they become highly significant when it comes to discussing legal support for ethical practice, including biomedical ethics.
Iranian criminal law, now known as the Law for Islamic Penalties, criminalises abortion, especially after ensoulment, and punishes professionals who carry out the procedure. The law also requires medical professionals to obtain informed consent for all medical interventions (except during emergencies). Breaching confidentiality can be punished with 91 days to one year of imprisonment. In addition, healthcare providers can be punished if patients are injured due to negligence (24). There are other laws, too, that require ethical standards in biomedical practices (25, 26, 27). Since 1979, biomedical ethics has come to be applied in important areas such as organ transplantation, ARTs, therapeutic abortion and embryonic stem cell research (28). Contrary to the claims that consider the absence of legislation as the major impediment to biomedical ethics in Iran (29), some aspects of biomedical practices have been justified by the health system through Islamic rulings (fatwas), or legislation.
Islamic perspectives on ARTs
Marriage is among the issues of foremost importance in Islam and having babies is considered to be a way of preserving the lineage. Known in Islamic literature as nasab, this is one of the main goals of Shari’a (30). In the Islamic context, children are related to their biological parents. Thus, most Islamic scholars accept the use of ARTs, such as artificial insemination with the husband’s sperm and finding a solution to infertility by using the gametes of legitimately married infertile couples as these are aimed at preserving the child’s lineage. Sunni scholars accepted the use of IVF in March 1980, when theSheikh of el Azha’r, the great religious seminary in Egypt, issued a fatwa supporting IVF (31).
However, there is no such consensus on methods that require the use of third-party gametes. Most Muslim jurists do not accept such methods, even if they are the only way to have a baby. They usually argue that sperm donation is against the famous Islamic rule of “protecting private parts” (Hifz-e-Forouj). While almost all Sunni scholars reject the idea of the use of sperm from men other than the infertile woman’s husband, some Shi’a jurists do permit the use of third-party sperm to solve the problem of infertility among married couples (32, 33, 34). As for egg donation, most Muslim scholars do not favour the practice as this, too, violates Hifz-e-Forouj. In view of the prevalence of polygyny, some jurists, both Sunniand Shi’a, allow a man to temporarily marry a woman other than his wife and use this woman’s egg if his wife is infertile (31). In such a situation, the issues of motherhood and lineage are decided by the usual rules and the child is considered to be the descendant of the biological mother, despite the views of some who have recently proposed a two-mother Islamic theory (35). Here, it is important to explain the difference between Sunni and Shi’ajurists’ opinions on temporary marriage. A temporary marriage is of limited duration. A man can marry a number of women for a predetermined period of time, after which the marriages dissolve. While Sunnis do not consider temporary marriage to be legitimate, Shi’ajurists deem it acceptable if the woman concerned is a widow. This facilitates the involvement of a third party for surrogate motherhood and egg donation, and provides a way to tackle some sensitive issues like intimacy, which is considered a precondition for legitimate conception by some jurists.
Similar problems exist with respect to surrogacy, despite the fact that generally, the Shi’aschool accepts this as a means of solving the problem of infertility. Most Sunni Muslim scholars do not permit surrogacy. Some believe that it should be allowed only in cases in which the zygote is to be implanted in the uterus of another wife (36). Among Shi’ascholars, the issue that is usually debated is which woman should be considered the mother – the woman who carried the baby in her uterus or the woman who donated the egg. In summary, the issues of egg donation and surrogacy are conceptually accepted as legitimate in the Shi’a Muslim world, and the main debates centre around legal issues, such as intimacy, lineage and the like.
ARTs and Iran’s legal system
Modern medicine made its entry in Iran in the 19th century through the establishment of the Dar-ul-Fonoon, the first modern university and institution of higher learning in Persia (37). The first Act for regulating medical practices was ratified in 1911 (38).
Child adoption is an option for infertile couples, but it may not be considered a perfect alternative to ARTs and is hardly a technology (39). On the other hand, some researchers hold that, “the rise of ARTs has undermined adoption and devalued its social meaning” (40). In 1975, Iran passed a law, the Law for Supporting Derelict Children, to legalise adoption. Some infertile couples have adopted children under the provisions of this law (41). This law can be labelled the first legal instrument for helping infertile couples in Iran. The law was abolished in 2013 and replaced by a new Act, The Law for Supporting Derelict Children and Adolescents. The Act permits the adoption of female babies by infertile couples who have remained childless after five years of marriage and if one of them is more than 30 years old; couples with children, with at least one of them being over 30 years old; and women who do not have a husband and are at least 30 years old. Among the other qualifications are that the applicants should have the requisite financial resources to raise a child, they should have an acceptable level of physical and mental health, they should not have a criminal record, they must be committed to religious and moral norms, and they should belong to one of the religions officially recognised by the constitution, including Islam, Christianity, Judaism and Zoroastrianism (42).
After the Islamic Revolution, the Iranian political and legal system changed dramatically and became the only one of its kind in the world. This was the first time in the history of the Shi’athat clerics became directly responsible for governing society and dealing with a range of executive and administrative issues, including health-related problems. The latter included the debate surrounding issues such as abortion and new emerging technologies, eg organ transplantation. In Iran’s political system, the views of the supreme leader form a religious justificatory basis for the ratification of laws and regulations. The Guardian Council validates laws which have been passed and through its supervision, ensures that they are compatible with Shari’a and the constitution.
Since the Iranian legislative system is based on the Shi’a school of Islam, fatwas can justify special practices, such as the use of ARTs, even in the absence of an officially ratified law. For this reason, it is important to clearly set out the Shi’a juristic views on the subject, which we have already done. However, the fatwa of one jurist may differ from that of another, even though they have the same jurisprudential sources, leading to a pluralistic discourse. Naturally, policy-making based on such different and even contradictory fatwas can create complications. The question arises as to which fatwa should be considered as the basis for legislation. When the issue is not overly contentious and a broad consensus exists among the religious scholars, it is this general opinion which is usually considered. However, when there is a lack of consensus, especially in the case of new emerging biomedical technologies, it usually takes a long time to arrive at a consensus. In some cases, it seems nearly impossible, and policy-makers must choose one of the juristic opinions. In the absence of an organised Shi’a seminary (like the Catholic church), the legislative system can enact laws on the basis of fatwas such as those issued by the supreme leader, whose opinion can form a sufficient ground for the justification of biomedical practices by the executive arm.
When Ayatollah Khomeini became the first supreme leader of Iran, the issue of ARTs had not come up in Iran. ARTs came into use once Ayatollah Khamenei, Ayatollah Khomeini’s successor, took over. His liberal opinions, unlike those of other Sunni and even Shi’a jurists, have paved the way for the development of assisted reproduction practices in Iran (43). His juristic ruling in 1999 permitted the donation of gametes by third parties to infertile spouses. However, he specified that the child would be related to the donor, either of the sperm or the egg, and not to the recipient couple. Although this fatwa has opened the way for many infertile couples to use third-party gametes (whether sperm or eggs), the recipients mostly hide the genetic background of the baby and sever relations with the donors. None of the official identity documents of the child contain any evidence of who the genetic parents are. It might be very hard, and even impossible, to trace the child’s genetic roots, in the absence of a reliable registry. Such use of ARTs, which is not clearly justified by the official laws, has become a source of real concern. The child’s right to know about his/her genetic roots has been seriously compromised (44). This fatwa is considered unique among Shi’a and Sunni jurists and is generally thought of as revolutionary, even among Shi’ascholars (45). IVF clinics offer gamete donation services in Iran under Ayatollah Khamenei’s original fatwa , and also in Lebanon, where he has many Shi’a followers. Ayatollah Khamenei also allowed the use of gametes after the death of their originator (43). There have been reports regarding the exchange of gametes for money in Iran and Lebanon, where some women sell their eggs to infertile couples. In addition, some Sunni infertile couples are secretly using third-party gamete donation services (46).
Iran Embryo Donation to Infertile Spouses Act (IEDISA)
Among all the ART methods that can potentially be performed in Iran due to the relative lack of restrictions under Ayatollah Khamenei, the only officially recognised one is embryo donation. The motion on IEDISA was tabled in Parliament on October 10, 2001, by 112 parliamentary representatives In keeping with the normal parliamentary procedure, it was sent to the related parliamentary commission, in this case, the Parliament Commission for Health, for primary evaluation.
On January 16, 2002, the motion was brought to the Public Hall of Parliament for the first time. The general concept was ratified and the motion was referred to the Parliament Commission for Health once more for a more detailed review and expert consultation (47). In the detailed discussions of the parliamentary representatives, those opposing the motion put forward several arguments against the motion. They cited the example of the commercialisation of kidney donation in support of their fear that the proposed provisions could result in “selling babies”. The need for greater adherence to juristic and Islamic principles, along with the need for more juristic fatwas, was also raised. In addition, they expressed doubts regarding the social and legal consequences of the Act once it was ratified and came into force. In this respect, the detractors of the motion were especially concerned about the Islamic rulings on heritage, intimacy and rule of lineage. On the other hand, the supporters of the motion emphasised the financial benefits of allowing this practice to be performed within the country. Further, they held that it would solve the problems of many families, promote scientific development in the country, decrease the prevalence of infertility-based divorce, and address the problems caused by the ambiguities in earlier laws, especially the Child Adoption Act, in the area of inheritance (48). They asserted that the proposed act could address the problem of intimacy by using the Islamic rule on the nursing of a baby, which too leads to intimacy (between the baby and the surrogate mother, her husband and children) (33). To convince the parliamentary representatives, there was also talk of the use of some unrealistic biotechnological innovations, such as inserting the genes of the requesting parents into the embryos so as to solve the problem of lineage, and the use of a computerised network to help prohibit marriage between siblings who do not know that they are related by blood.
While the motion was being discussed in parliament, the Guardian Council began deliberating on the proposed act prospectively, while normally the Guardian Council starts its check after finishing the ratification process in the parliament (49). The proposed act was brought to the Public Hall of parliament for the second time on August 27, 2002, but was not accepted by the Guardian Council (50), and for the third time on June 8, 2003 (51). The law was finally ratified on July 20, 2003 (52), though several parliamentary representatives were still concerned about the issues of inheritance, intimacy and the marriage of such children (53).
According to the first article of the Act, all authorised infertility clinics may transfer an embryo resulting from IVF – provided it is the embryo of a legally and juristically legitimate couple – to the woman’s uterus in the case of couples whose infertility has been proven following medical treatment. The written consent of the couple is required for this procedure. This Act covers bilateral and unilateral infertility in both men and women. In summary, the Act permits all infertile couples to receive embryos, provided the woman can potentially carry a foetus within her womb.
The second article of the Act declares that a couple which wants an embryo should make a request to the court, which will be responsible for evaluating the couple’s eligibility and competency. The process of donation should start only after the court has granted the couple permission upon ascertaining that they are morally fit and hold Iranian citizenship. This article specifies that the couple should not be legally incompetent, must not abuse or be addicted to drugs, and should not be seriously ill.
Other parts of the law emphasise the responsibilities of the couple towards the coming child. These are the same as in the case of normal parents, and pertain to the care and education of the child, alimony and respecting the child (Article 3). Cases related to couples who make a request for embryos are given priority in the family courts, and procedural formalities are not observed. Further, the cases of couples who have been disqualified by the family courts may be reconsidered (Article 4).
Finally, the last part (Article 5) of the Act tasked the MOHMEwith preparing the Executive Bylaw of the Act within three months, with the cooperation of the Ministry of Justice, for ratification by the Council of Ministers.
The Executive By-law of IEDISA
The Executive By-law of the Act was passed by the Council of Ministers on March 13, 2005 (54). According to the bylaw, donation should be voluntary and should not involve any monetary exchange. The embryos of officially married couples could be used if the age of the embryos is less than five days after conception. According to this bylaw, the physical and mental health and intelligence quotient (IQ) of the donor couple should be normal; they should not be addicted to or abuse drugs; and they should not be suffering from serious diseases such as HIV/AIDS and hepatitis. In addition, preserved embryos should be classified on the basis of their parents’ religion, especially into Muslims and non-Muslims, to maintain a religious balance between the donors and recipients. This part of the by-law emphasises the confidentiality of the process of obtaining, preserving and donating embryos. Such information is termed “top secret governmental documents” and may be disclosed only on a court order. Finally, the by-law permits the establishment of embryo banks under the supervision of the MOHME.
The process of receiving donated embryos
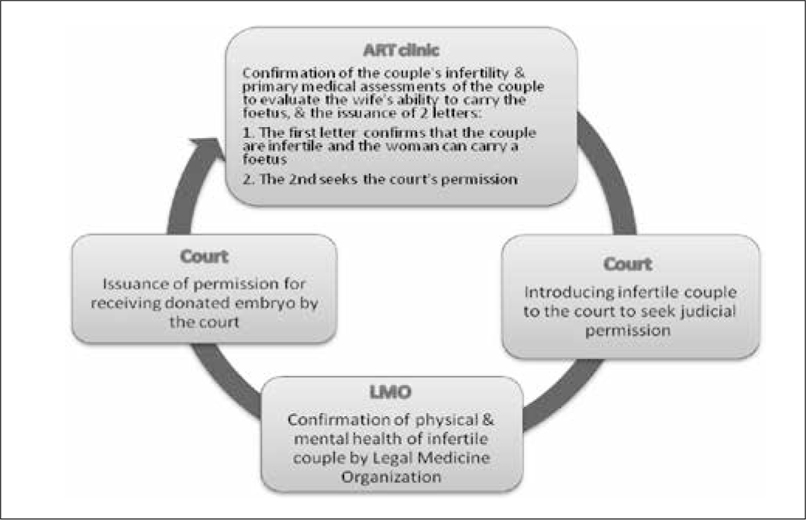
Today, infertile couples in need of donated embryos must first visit an infertility clinic for a primary medical assessment. This is necessary as their infertility needs to be established. At this stage, it is ascertained whether the wife can potentially carry a foetus in her womb, whether both or one of the spouses are completely infertile, and if other methods cannot be used. After clarifying these points, the infertility clinic introduces the couple to the court to seek the court’s permission. Simultaneously, the clinic sends the results of the investigations regarding the couple’s infertility and the wife’s ability to carry a foetus to the Legal Medicine Organisation (LMO). The court then refers the couple to the LMO. Here, the couple presents the clinic’s reference letter, which provides a confirmation of infertility and the woman’s ability to carry a foetus. At the LMO,the couple undergoes physical and mental examinations, and the competency of the two to receive donated embryos is evaluated. The results of the LMO evaluation are sent to the court and the judge decides on whether an embryo may be donated to the couple. Finally, if the court sees it fit to allow the couple to receive a donated embryo, it conveys its decision to the infertility clinic (55).
Fig. 1: The process of obtaining permission for the receipt of donated embryos in Iran
MOHME Guidelines for Regulation of ART Clinics
In 2010, the MOHMEreleased draft guidelines (56, 57) for the regulation of ART activities in the clinical setting. These included the guidelines on Health Evaluation in Embryo and Egg Donation and Required Evaluations for the Treatment of Infertility through Gestational Surrogacy. Although the content of these two sets of guidelines pertains mainly to the technical, medical and clinical assessment of the donor and recipient couples, such as andrological, endocrinological, urological, obstetric, gynaecological and embryological evaluations, it also includes a series of recommendations related to the ethical and legal aspects of the practice. Even though these guidelines were prepared and sent to ART clinics, as well as to a list of experts in the form of a draft for their feedback in 2010, they have still not been officially released by the MOHME. Some ART clinics use these drafts as an unofficial document, mainly because they do not have any other official basic regulations.
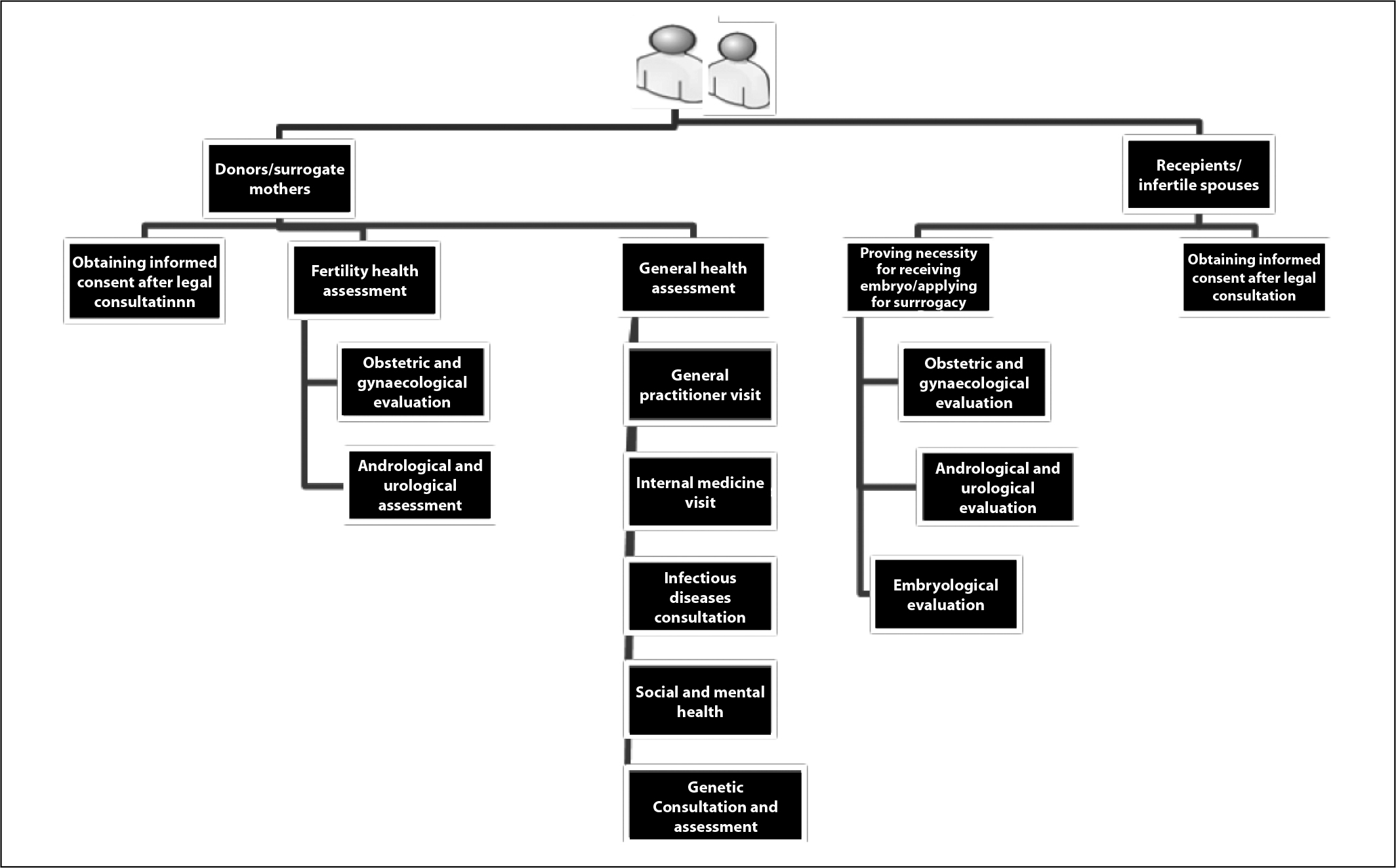
The first draft guidelines, Health Evaluation in Embryo and Egg Donation, prescribe that all decisions regarding medical and technical interventions should be guided by ethical and legal consultants to help infertile couples make decisions that are compatible with moral/jurisprudential norms and legal regulations. The issues that donor couples need to consider during counselling sessions are confidentiality, honesty and altruism. In addition, this draft guideline recommends that the couple should seek a fatwa to ensure that the intervention is permissible under the religious decree of the cleric they follow (marja’taqlid). The other measures recommended by the guidelines in the case of donor couples are legal consultations, obtaining informed consent, and assessment of their social and mental health status. The last measure names criteria for the refusal of candidates for embryo/egg donation. These include illiteracy, disabling anxiety, substance abuse, any type of personality disorder, an IQ that is lower than normal, a positive criminal record, instability in spousal relationships, instability in decision-making, a positive history of attempted suicide, psychiatric problems passed down genetically (eg schizophrenia, obsessive-compulsive disorders, depression and bipolar disorder), and high-risk sexual behaviour or having multiple partners.
In addition to medical and technical evaluations, the guidelines recommend counselling sessions for couples applying for embryos/eggs. The issues to be considered during the initial consultation and assessment of the couple are: their social status in terms of their educational level, their economic status (job/livelihood), the stability of the relationship between the spouses, the integrity of the family’s foundation, previous marriages and divorce records, whether they have had a child previously or have an adopted child, if either party has a positive criminal record, (if they are ready for) the mental and social effects of having a child, the ethical and legal aspects of the procedure, and confidentiality. Emphasis should be laid on the need for honesty on the part of the couple. As for legal consultation and the matter of obtaining informed consent, the draft guidelines recommend that the legal norms, the obligations and responsibilities of the recipient couple, the principle of confidentiality, and the effects and outcomes of the procedure be considered thoroughly by a legal expert.
In general, “surrogacy” or “surrogate motherhood” is a complex issue from a cultural and legal standpoint in Iran (14), but nowadays, it is practised (36). Surrogacy is allowed on the basis of Shi’a jurisprudence, whereas the Sunni school does not permit it (58). There have been reports of ethical problems related to the financial transactions involved (59), but this seems to be acceptable among infertile women (60). As in the case of most reproductive technologies in Iran, there is no legislative framework for surrogacy. The only guidelines provided by the MOHME on this matterare the “Required Evaluations for Treatment of Infertility through Gestational Surrogacy”. Under these guidelines, the couple seeking treatment and the potential surrogate mother and her husband are assessed medically, as well as in moral terms. The guidelines recommend that to determine whether surrogacy treatment should be allowed, ART clinics must ascertain the social and economic status of the couple, using indicators such as unemployment, the stability of the couple’s relationship, integrity of the family’s foundation, applicants’ mental health status, previous marriages and divorces, whether the couple has had a child earlier or has an adopted child, substance abuse, and whether either party has a positive criminal record.
A number of additional issues are to be considered in the initial assessment of the surrogate mother and her husband (when the woman is married), such as religious issues, the motives of the woman who wants to become a surrogate mother, her level of awareness of the treatment process (including her awareness of the problems that may arise during the treatment), and her mental health status.
Discussion
Need for more comprehensive regulatory measures
Today, the most important criterion for eligibility for ARTs in Iran is being legitimately married. In other words, if a man and woman are officially married, they can make a request for all possible methods and ART technologies to have children, even if one of them has changed his/her sex because he/she was a transsexual. (Sex reassignment surgery is legal in Iran. The person concerned is given a new name and the previous gender is not mentioned. Transsexuals are allowed to marry after the surgery). Some juristic rules and principles, such as those related to preserving the lineage, guarding the private parts and protecting the sexual organs, are no longer concerns in Iran today, officially or practically. The openness regarding the use of ARTs and the lack of comprehensive regulatory measures have led to a certain level of confusion and ambiguity (61). Even though various ARTs are used in Iran, the only method that is regulated by an official law is embryo donation. As a result, each ART clinic has its own regulations, which are usually not transparent.
Fig. 2: Required qualifications of embryo donors/surrogate mothers and recipients/infertile spouse (MOHME draft guidelines)
IEDISA and the Executive By-law: legal and ethical problems
Although the ratification of the IEDISA and its bylaw may be considered a positive development, the Act can be criticised from various angles. From the legal point of view, the Act does not clarify the legal status of lineage. Although it lays down that the responsibilities and commitments of the recipient couple towards the baby are like those of normal parents towards their children, it does not clarify that they are parents. Although the Executive By-law requires ART clinics to confirm the identity of donor couples and considers this information as top secret, the events following the transfer of the embryo into the uterus of the recipient woman are not covered by the law and the Executive By-law. So just after the transfer of the embryo, the receiving couple usually leaves the ART clinic forever. The woman can give birth to the baby at any medical facility of the couple’s choice and the baby would be registered officially in the pregnant woman’s and her husband’s official documents as their child. Therefore, despite the original Fatwa and also the legal system that still considers the genetic relation the most important connecting issue, this act ignores the embryo donors. This leads to ambiguity as far as the concept of intimacy, between the child, recipient couples, and their relatives, is concerned. Here intimacy is a technical Islamic word that is used to show which relatives are intimate to the person. It is important because intimate relatives cannot marry each other and observing the Islamic dress code for women (Hijab) is not obligatory among intimate relatives.
Inheritance is another important issue that is not clearly mentioned in this law. While the law is clear about some of the recipient couple’s responsibilities, such as respecting and caring for the child, providing him/her with an education, and alimony, the issue of inheritance is not clearly mentioned. Since the present system requires the baby to be officially registered as the child of the recipient couple, and considering that most couples take recourse to embryo donation in a very secretive manner, the child inherits from the recipient couple. However, it is possible to imagine a situation in which one or both of the recipient parents deny the child an inheritance, using the argument that the child is not their genetic offspring
Although the evaluation of donors, mentioned in the by-law, consists mainly of a medical assessment to be performed by the ART centre, a problem that the court may encounter relates to the assessment of the moral competence of the recipient couple. Usually, it is very hard to draw up a set of criteria for moral competence. Neither the law, nor the by-law gives a satisfactory definition of moral competence, and it seems that the courts have to decide for themselves if the parents are morally competent. This may result in conflicting court decisions in similar cases. Moreover, limitations could be imposed on certain social groups as a result. Couples who are refused by the court on the ground of being morally incompetent could be stigmatised and discriminated against.
Another problem is that the law places no limit on donation. Because of this, together with the absence of a registry system, it is not clear how many times a person has donated (62). This acquires considerable importance in a society which is very sensitive about the issue of intimacy, as stated above, intimate relatives, according to the religion and tradition, cannot marry each other . In addition, there is a double standard with respect to nationality: while the law pays no attention to the nationality of the embryo donors, it stipulates that the recipients be Iranians. The legislation thus denies other nationalities the opportunity to receive such treatments, even though nationality is not an ethically relevant issue in the provision of medical care according to the ethical standards of medical practice in Iran, including the Iran Patients’ Rights Charter (63) and Medical Code of Conduct (64). This article of the law neglects millions of Afghan refugees and migrants who live in the country (65).
In the case of almost all ARTs using donated gametes and embryos, the right of the children to know their genetic roots is another important issue that is neglected in Iran. Although according to the Law for Supporting Derelict Children and Adolescents, the child’s lineage should be recorded and the genetic parents’ names must be mentioned in the child’s identity card (42), the IEDISA, which is the only official law dealing with ARTs, and the Executive Bylaw are silent on this important issue. Thus, there is no guarantee that the recipient couple will tell the child the truth about his/her genetic roots at any point in his/her life. In addition, although the IEDISA by-law considers the genetic information regarding the donated embryo top secret and stipulates that the documents containing such information be maintained at the ART centre, these documents are rarely available and access to them requires special permission from the judiciary. The situation is still more complicated in the case of gamete donation because ART centres providing this service to infertile applicants are not legally mandated to keep any records of the donors. This blind gamete donation system is conducive to the proliferation of professional donors and also works in favour of recipient couples who prefer to keep the baby’s genetic roots a secret. Such couples are secretive about the baby’s genetic roots because this helps them to avoid social pressures and the stigma of being infertile. Thus, the child’s right to be aware of his/her genetic lineage is given no importance. While the child as the main person is usually denied knowledge about his/her lineage, several persons and organisations including the ART clinic and court staff are involved in the embryo donation process, since the principle of confidentiality is potentially at stake.
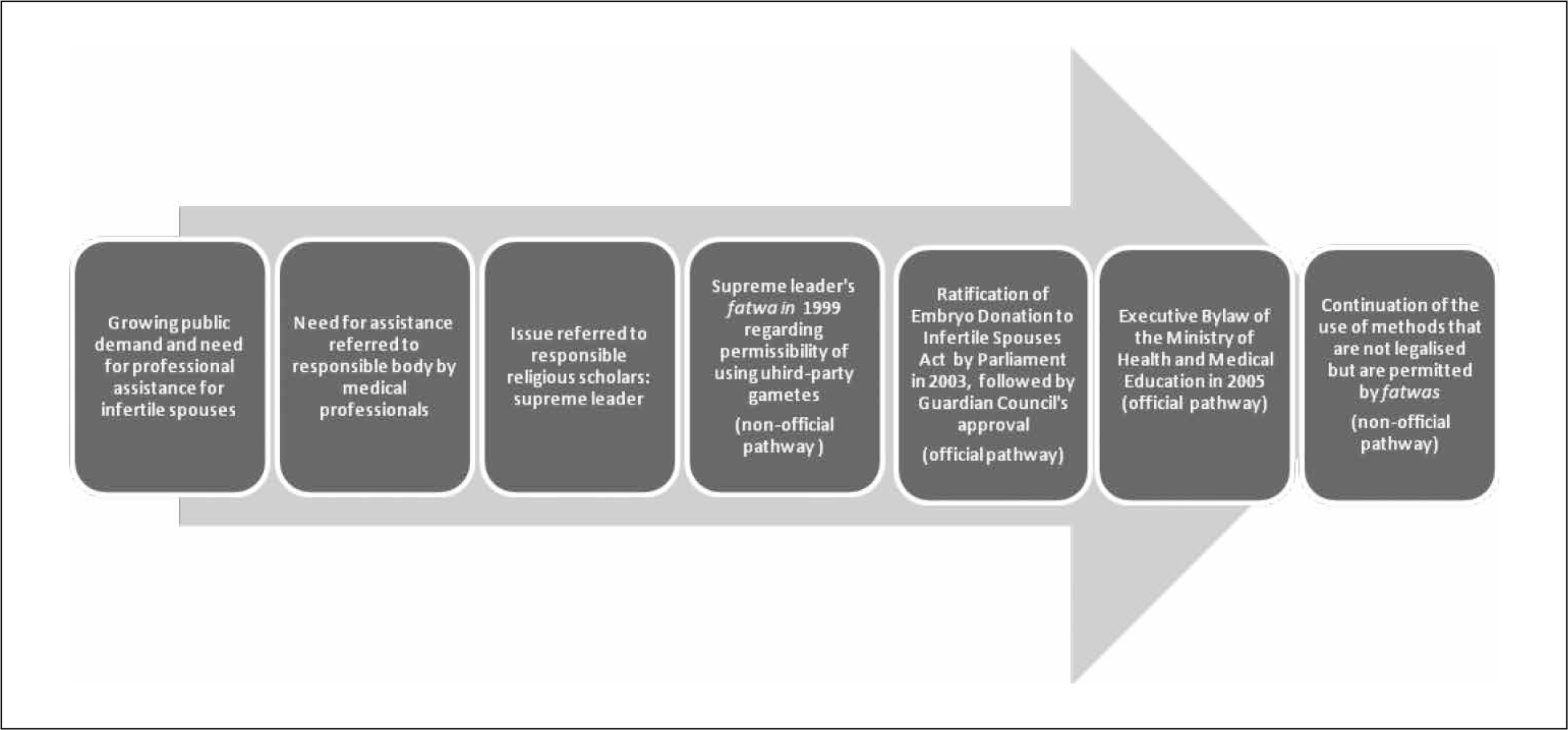
Fig. 3: The process of legalisation of assisted reproduction in Iran
Another problem with the Act and Executive By-law is that both the donor and recipient couples are evaluated not only medically, but also with regards to the recipient couples’ social, mental and physical health and economic status. For example, they are supposed to be tested to rule out substance abuse, a not infrequent problem among Iranian adults. It seems it is felt that such preconditions will guarantee the maximum familial support for the baby, but on the other hand, limiting the access of such groups to ARTs cannot be easily justified from an ethical point of view. It is very hard to say that conditions such as poverty and addiction warrant depriving such persons of medical treatments such as ARTs and ignoring the “right to fertility and child bearing”.
Such a view puts the ethical principle of justice at stake. Further, it could lead to discrimination against and stigmatisation of such social groups. In summary, it could be said that there is an innate paradox in this law even with respect to the provision of support to the child. On the one hand, the socioeconomic and heath status of the applicants is evaluated to ensure sufficient familial support for the child, but on the other, no importance is given to the child’s right to know about his/her genetic roots
The process of legalising an ethically sensitive issue after 1979
Two pathways have played a substantial role in justifying the use of ARTs, which is a highly sensitive issue both from the religious and ethical points of view. The first pathway, which we shall call the “non-official pathway”, is based on the supreme leader’s fatwas. The process starts with a public request from medical professionals, who comprise the first line in responding to such needs. These professionals naturally seek justified ways, including suitable laws, of responding to those needs. In the absence of an official law, a practice may be justified by the supreme leader’s fatwa, which could serve as an unwritten law, paving the way for the ratification of official laws by Parliament and guaranteeing approval of the law by the Guardian Council.
After a period of practising ARTs and attempting to create a conducive sociopolitical atmosphere, the medical professionals who held governmental positions tabled the bill of IEDISA in Parliament. This process we call the “official pathway”. The final step would be notification of a by-law by the executive or judiciary branches of the government. It is important to mention that IEDISA has only legalised one of the various methods of ARTs and the “non-official pathway” has again continued in order to justify other ART methods.
Need for a rule-based juristic approach
Unlike Iran’s Therapeutic Abortion Act, based on the Islamic jurisprudence rule known as La Haraj, which addresses the concept “no unbearable burden should be imposed on a Muslim” or the juristic rule that addresses “protection against distress and constriction” (el-‘ausrwava el-haraj) (28), no such principle-based approach has been adopted in the case of ARTs. It is important to use an approach which employs the language of rules and principles in contemporary Islamic biomedical ethics, given that most fatwas and the consequent laws have traditionally been unilateral and subjective. In addition, the lack of such an approach, as well as the absence of an organised seminary, has resulted in a number of discrepancies in related areas and hindered education in and deliberation on biomedical ethics. Therefore, the adoption of an approach that uses the language of principles and rules could be a very good starting point for the development of a more normative system for Islamic biomedical laws and ethics.
Conclusion
The fact that Shi’a clerics were given the responsibility of governing society and responding to public needs by issuing positive fatwas to widen the range of permissible assisted reproduction methods may have played a central role in the framing of laws and in influencing the judiciary. Such fatwas would pave the way for legalising sensitive issues, such as embryo donation. The IEDISA is an example of the fact that such issues can be legalised in the contemporary politico-legal milieu in Iran.
It is very important to carry out investigations in the future to evaluate ART practices in Iran, as there is a need for reliable information on any problems with the existing dispensation. Such research would provide the necessary underpinning for a more comprehensive and ethically justified legal framework for ARTs.
Acknowledgement
We would like to express our gratitude to the Kennedy Institute of Ethics and Bioethics Research Library at Georgetown University, Institute of Biomedical Ethics and History of Medicine at the University of Zurich. We would also like to acknowledge the contributions of Dr Mahmoud Abbasi and other colleagues at the Iranian Research Center for Ethics in Law and Medicine at Shahid Beheshti Medical University, as well as Dr Asiyeh Jafari from the LMO.
References
- Abbasi-Shavazi MJ, Inhorn MC, Razeghi-Nasrabad HB, Toloo G. The “Iranian ART Revolution”: infertility, assisted reproductive technology, and third-party donation in the Islamic Republic of Iran. Journal of Middle East Women’s Studies. 2008 spring; 4(2):1-28.
- Berek JS, Novak E. Berek and Novak’s gynecology. 14th ed. Philadelphia: Lippincott Williams and Wilkins; 2011.
- Fardiazar Z, Amanati L, Azami S. Irrational parenthood cognitions and health-related quality of life among infertile women. Int J Gen Med. 2012;5:591-6.
- Aliyeh G, Laya F. Quality of life and its correlates among a group of infertile Iranian women. Med Sci Monit. 2007 Jul;13(7):CR313-7.
- akpour AH, Yekaninejad MS, Zeidi IM, Burri A. Prevalence and risk factors of the female sexual dysfunction in a sample of infertile Iranian women. Arch Gynecol Obstet. 2012 Dec;286(6):1589-96.. doi: 10.1007/s00404-012-2489-x. Epub 2012 Aug 1.
- Vahidi S, Ardalan A, Mohammad K. Prevalence of primary infertility in the Islamic Republic of Iran in 2004-2005. Asia Pac J Public Health. 2009 Jul;21(3):287-93.
- Safarinejad MR. Infertility among couples in a population-based study in Iran: prevalence and associated risk factors. Int J Androl. 2008 Jun;31(3):303-14.
- Ahmadi Asr Badr Y, Madaen K, Haj Ebrahimi S, Ehsan Nejad AH, Koushavar H. Prevalence of infertility in Tabriz in 2004. Urol J. 2006 Spring;3(2):87-91.
- Marzieh N. Epidemiology of infertility in the west of Tehran in 2000. J Am Med Womens Assoc. 2002 Fall;57(4):219.
- Akhondi MM, Kamali K, Ranjbar F, Mahdi SHIR, Shafeghati S, Ardakani ZB, Goodjani A, Parsaeian M, Mohammad K. Prevalence of primary infertility in Iran in 2010. Iranian Journal of Public Health. 2013;42(12):1398-404.
- Andersen AN, Gianaroli L, Felberbaum R, de Mouzon J, Nygren KG. Assisted reproductive technology in Europe, 2001. Results generated from European registers by ESHRE. Hum Reprod. 2005 May;20(5):1158-76. Epub 2005 Jan 21.
- Inhorn MC. “He won’t be my son”: Middle Eastern Muslim men’s discourses of adoption and gamete donation. Med Anthropol Q. 2006 Mar; 20(1):94-120.
- Clarke GN. ART and history, 1678-1978. Hum Reprod. 2006 Jul;21(7):1645-50.
- Henig RM. Pandora’s baby: how the first test tube babies sparked the reproductive revolution. Cold Spring Harbor, N.Y.: Cold Spring Harbor Laboratory Press; 2006.
- Cohen ME. The “brave new baby” and the law: fashioning remedies for the victims of in vitro fertilization. Am J Law Med. 1978 Fall;4(3):319-36.
- Sadeghi Moghadam MH. Juridical Basis and Legal Requirements of Embryo Donation Act. Nameh Mofid. 2004;10:31-60. Persian
- The first baby resulted from IVF in Iran [Internet]. Official Website of Royan Institute [Cited 2013 Feb 15]. Available from: http://www.royaninstitute.org/cmsfa
- Afshar L, Bagheri A. Embryo donation in Iran: An ethical review. Dev World Bioeth. 2013 Dec;13(3):119-24.
- Tremayne S. Law, ethics, and donor technologies in Shi’a Iran. In: Assisting reproduction, testing genes: global encounters with new biotechnologies. Birenbaum-Carmeli D, Inhorn MC (eds). New York: Berghahn Books; 2009:144-63.
- Ministry of Health and Medical Education. Regulation for Establishment of Assisted Reproductive Technology Clinics.MOHME, Islamic Republic of Iran; 2006.
- The Constitution of Islamic Republic of Iran [Internet]. August 8, 2012. Persian. Available from: http://rc.majlis.ir/fa/content/iran_constitution
- Iran Public Insurance Law [Internet] October 24, 1994. Available from: http://rc.majlis.ir/fa/law/show/92470
- Iran Civil Code [Internet]. May 8, 1928. Persian. Available from: http://rc.majlis.ir/fa/law/show/97937
- Law for Islamic Penalties [Internet]. July 29, 1991. Available from: http://www.dastour.ir/brows/?lid=143178
- The Law for Prevention of Transmissible and Sexually Transmitted Diseases [Internet] [Cited June 9, 1941]. Available from: http://rc.majlis.ir/fa/law/show/90500
- The Law for Punishment of Avoiding Helping Injured People and Removing Life-Threatening Situation [Internet]. No. 8869, May 25, 1975. Persian. Available from: http://rc.majlis.ir/fa/law/show/97285
- The By-law for Punishment of Avoiding Helping Injured People and Removing Life-Threatening Situations, [Internet]. No. 84054, Jan 4, 1986. Persian. Available from: http://rc.majlis.ir/fa/law/show/109183
- Aramesh K. Iran’s experience on religious bioethics: an overview. Asian Bioethics Review. 2009 Dec; 1(4):318-28.
- Zali MR, Shahraz S, borzabadi S. Bioethics in Iran: legislation as the main problem. Archives of Iranian Medicine. 2002 Jul;5(3):136-40.
- Sachedina A. Islamic biomedical ethics: principles and application. New York: Oxford University Press; 2009:p103.
- Inhorn MC. Making Muslim babies: VF and gamete donation in Sunni versus Shi’a Islam. Cult Med Psychiatry. 2006 Dec;30(4):427-50.
- Khamenei A. Ajwibat el-istiftaift. Beirut: al-Dar al-Islamiyya; 2003:p69. Arabic.
- Larijani B, Zahedi F. Ethical and religious aspects of gamete and embryo donation and legislation in Iran. J Relig Health. 2007;46:399-408.
- Ayatollah Khamenei’s Juristic Opinions (Fatwa) Regarding Assisted Reproduction Technologies [Internet]. The Official Website of the Center for Preserving and Publishing the Works of Grand Ayatollah Sayyid Ali Khamenei; August 15, 2012 [cited 2015 Apr 4]. Persian. Available from: http://farsi.khamenei.ir/treatise-content?uid=21&tid=3
- Merghati ST. Lineage from artificial insemination with foreign interference. Maqalat Va Barresiha. 2005;75:125-48. Persian.
- Serour GI. Islamic perspectives in human reproduction. Reprod Biomed Online. 2008;(17 Suppl 3):34-8.
- Ekhtiar M. Nasir al-Din Shah and the Dar al-Funun: the evolution of an institution. JISIS. 2001;34(1/4):53-163.
- Bayat M. Iran’s first revolution: Shi’ism and the constitutional revolution of 1905-1909. New York: Oxford University Press; 1991.
- The Act for Medical Practice [Internet]. Jun 2, 1911[cited 2015 Apr 4]. Persian. Available from: http://rc.majlis.ir/fa/law/show/90145
- Blanchy S. [Adoption: an alternative to assisted reproductive techniques?]. Gynecol Obstet Fertil. 2011 Sep;39(9):491-5. French.
- Appleton SF. Adoption in the age of reproductive technology. Univ Chic Leg Forum. 2004;2004:393-451.
- The Law for Supporting Derelict Children [Internet], No 8819. Mar 20, 1975[cited 2015 Apr 4]. Persian. Available from: http://rc.majlis.ir/fa/law/show/97234
- Clarke M. Children of the Revolution: Ali Khamenei’s ‘liberal’ views on in vitro fertilization. British Journal of Middle Eastern Studies. 2007 Dec; 34(3):287.
- Khamenei SA. Question 1271-1277. Ajwibat el-istiftaift. Tehran: Amirkabir; 1999:2819. Arabic.
- Clarke M. Islam, kinship and new reproductive technology. Anthropology Today. 2006 Oct; 22(5):17-20.
- Inhorn MC. Globalisation and gametes: reproductive ‘tourism,’ Islamic bioethics, and Middle Eastern modernity. Anthropol Med. 2011 Apr;18(1):87-103.
- The Public Hall Detailed Discussions of 186th Open Session of The 6th Parliament of Islamic Republic of Iran [Internet]. 16599. Jan 16, 2002. p. 22-7. Persian. Available from: http://www.ical.ir/index.php?option=com_mashrooh&view=session&id=2716&Itemid=38
- The Law for Supporting Derelict Children [Internet]. Public law no. 8819, enacted March 20, 1975. Available from: http://rc.majlis.ir/fa/law/show/97234
- Report of the Prospective Expert Session of Guardian Council of Islamic Republic of Iran Research Center Research Center for Embryo Donation to Infertile Spouses Act [Internet]. Weblog of Ferdowsi University Association of Jurisprudence and Law.2002 [cited 2012 Aug 14]. Available from: http://www.aef.blogfa.com/post-17.aspx
- The Public Hall Detailed Discussions of 244th Open Session of the 6th Parliament of Islamic Republic of Iran [Internet]. August 27, 2002 [cited 2015 Mar 23]. Available from: http://www.ical.ir/index.php?option=com_mashrooh&view=session&id=2716&Itemid=38
- The Public Hall Detailed Discussions of 328th Open Session of the Parliament of Islamic Republic of Iran [Internet]. Jun 8, 2003 [cited 2015 Mar 23]. Available from: http://www.ical.ir/index.php?option=com_mashrooh&view=session&id=2540&Itemid=38
- Iran Embryo Donation to Infertile Spouses Act. Public law no 17033 [Internet]. July 20, 2003 [cited 2015 Mar 23]. Available from: http://rc.majlis.ir/fa/law/show/93943
- The Public Hall Detailed Discussions of 340th Open Session of the Parliament of Islamic Republic of Iran [Internet]. July 20, 2003 [cited 2015 Mar 23].. Available from: http://www.ical.ir/index.php?option=com_mashrooh&view=session&id=2552&Itemid=38
- Iran Embryo Donation to Infertile Spouses Bylaw [Internet]. March 13, 2005. Available from: http://rc.majlis.ir/fa/law/show/125235
- Jafari A. Personal interview with the author on the process of using embryo donation method by infertile spouses in Iran. November 5, 2013.
- Ministry of Health and Medical Education. Draft guideline for Assisted Reproductive Technologies: No 1, Health evaluation in embryo and egg donation. MOHME, Islamic Republic of Iran; 2010.
- Ministry of Health and Medical Education. Draft guideline for Assisted Reproductive Technologies: No2, Required evaluations for treatment of infertility through gestational surrogacy. MOHME, Islamic Republic of Iran; 2010.
- Serour GI. Islamic perspectives in human reproduction. Reprod Biomed Online. 2008;17 (Suppl 3):34-8.
- Aramesh K. Iran’s experience with surrogate motherhood: an Islamic view and ethical concerns. J Med Ethics. 2009 May; 35(5):320-2.
- Rahmani A, Sattarzadeh N, Gholizadeh L, Sheikhalipour Z, Allahbakhshian A, Hassankhani H. Gestational surrogacy: Viewpoint of Iranian infertile women. J Hum Reprod Sci. 2011 Sep;4(3):138-42.
- Samani RO, Moalem MRR, Merghati ST, Alizadeh L. Debate in embryo donation: embryo donation or both-gamete donation? Reprod Biomed Online. 2009;19 (Suppl 1):29-33.
- Mohammadi M. Marriage alimony and obedience. Motaleat Rahbordi Zanan. 2004;( 25):1800anan. Persian.
- Safaee SH. Deficiencies of Iran legal system regarding gamete and embryo donation from the comparative law perspective. Payesh Quarterly. 2007;6(4):3234. Persian.
- Alavi Ghazvini SA. Describe and assess the embryo donation law. Thoughts of civil law. 2009; 5(12):141-64. Persian.
- Jabari M. Some ambiguities in the Embryo Donation Act. Semnan University Journal. 2008;6(19): 107-115. Persian.